DR. KOCH WAS not idle during the many years of Government investigations and trials. He cooperated with any scientific group, which indicated it was anxious to find out the truth in all honesty.
Up in British Columbia, Canada, the Provincial Government carried on a five-year investigation of the Koch Treatment in animal work. The dairymen asked the Provincial Government to find out if this Treatment would help eliminate such costly diseases as Bang’s disease, mastitis, etc. Each year thousands upon thousands of cattle die from these ailments, and nothing has been found to counteract this wide destruction.
Each year the Department of Agriculture came out with an interim report. In 1948 the final report was released. This was but another link in the chain of evidence, which supported the already widespread experience of thousands of people that the Koch Treatment had definite therapeutic value, and in many cases, was superior to the existing “approved” methods used by the AMA.
Experts from the British Columbia Government, as well as the University of British Columbia testified in the trial of Dr. Koch. Physicians who used hundreds and even thousands of these Treatments were put on the witness stand. Each one of them depended for success in his individual practice on the things they used to treat disease. If the Treatment were ineffective, they could not afford to use it.
Contrast this type of evidence with that presented by the Government with the help of the AMA. The rebuttal of facts such as are presented in Part Two of this book, was impossible. Only fact testimony can refute a statement, which is a fact. And, as the facts required for rebuttal do not exist, the Government must have realized that it would have to depend on “opinion” Testimony. Dr. Koch, of course, had no defense against “opinion” Testimony. This “opinion” Testimony was given by experts, supplied by the AMA who had never really used the Treatment, and knew nothing about its chemical actions in the body. Such experts were chosen because of the impression they may give and so convince the jury that the scientific world is against the defendant, as well as the Government, itself.
GOVERNMENT ATTACKS REPUTATIONS OF KOCH SUPPORTERS
Another feature of the trial was for the Government attorneys to attempt to attach derogatory and false accusations upon the witnesses for Dr. Koch. The case of Dr. Hendricks, mentioned elsewhere, is an example here.
Dr. Hendricks had treated a far advanced case of cancer involving both the breast and uterus. This woman had received treatment in vain from various doctors and hospitals, and as the disease advanced, it caused intense pain, which necessitated taking large doses of opiates. She was brought to Dr. Hendricks in this condition, depleted financially and physically, a subject of pity.
Dr. Hendricks treated her as a charity case with the Koch Treatment and had to prescribe, morphine also, because of the pain. After her recovery was completed so far as one could tell from physical examination, she still complained of pain. Thereupon, Dr. Hendricks wrote the Narcotics Division of the Government requesting them to advise him what to do in such a case, because the patient complained of pain and he could find no physical cause for it any longer. He did not want to prescribe morphine under such circumstances.
Instead of giving this advice, which was their duty, they waited until Dr. Hendricks was testifying on the witness stand for Dr. Koch; then they attempted to frame him as a dope peddler. Mr. Gallagher, the defense attorney, saw through their trick and demanded that they produce the letter, which Dr. Hendricks wrote asking for advice. They saw that this would immediately defeat their purpose and hurried from the subject, glad to escape it.
Such low attempts to smear the witnesses were tried on several witnesses for Dr. Koch. They were to take the place of facts in the attempt to wipe out truths that humanity has long needed.
NEWSPAPERS REPORT ONLY GOVERNMENT’S TESTIMONY
By the summer of 1946, the trial was over. It was the longest in the history of the Food and Drug Department. Even the newspapers in Detroit cooperated 100 percent with the AMA. For five weeks of Testimony by Government witnesses, an article appeared each day denouncing the Treatment. Dr. Koch’s defense began in the middle of the week. The articles stopped. His defense lasted for months, but no one knew about it unless they were in the courtroom.
(The clippings, which are in the rear of this book, are all taken from the first trial in 1943.) The AMA discovered that there might be some regard for Koch with such articles, and evidently ordered that all news be “blacked out” in the second trial. The press wires were never permitted to print one story, although this was a trial affecting every person in the world, and besides, was the longest in the history of the Food and Drug Department.
Rumors were spread around official circles that the Government attorneys were working for a third trial, which, if it had happened, would have been the first time in the history of our country.
A few months after the trial was all over, ironically enough, one of the attorneys for the Government who had fought the Treatment with a vengeance, died of cancer in an AMA hospital. (During the trial, Dr. Koch had noticed a lump on his neck, and being concerned that it was malignant offered to treat him, but was coldly rebuffed.)
For two more years the Government left Dr. Koch hanging in the air. Twice, in more than three years, the opposition had failed in establishing its charges. Meanwhile, tremendous public interest was being built up.
Larger and larger numbers of Christian preachers were becoming interested in the cause, which this Treatment represents. Dr. Koch has had an established rule that any person of any Christian persuasion who was serving the cause of Christ would receive gratis Treatment at his Clinic.
It was his way of saying “thanks” to his Lord and Savior for the many blessings, which He has endowed, on this work. Recoveries were reported all over the nation. Yes, some were not able to affect a recovery. In cancer cases, they were frequently burned by radiation, or rendered hopeless by constant cutting and probing. Others came too late, after trying everything else first. However, impossible cases were nevertheless, making recoveries; cases diagnosed by others, were cured by the Koch Method. In high and low places in the Christian church, men were coming to know about this work. Toward the close of the Eightieth Session of the United States Congress, in 1948, Senator William E. Langer of North Dakota placed an article into the Congressional Record, which contained factual information regarding the Treatment. Copies of this article were distributed over the nation. The Senator had made an independent investigation of Koch Therapy several years earlier. Instances are now recorded of lives having been saved through knowledge disseminated, resulting from Senator Langer’s courage.
(The clippings in the rear of the book also contain others. Those which speak of a court trial and are rubber stamped “1943” are referred to at this point.)
On August 17 1948, a truly surprise decision was carried on the front page of the Detroit Times, as a “late flash” news item. The next day all three Detroit papers carried the story. Here is the one, which appeared in the news:
“U. S. QUASHES KOCH CHARGES”
“Dismissals Follow Two Lengthy Trials”
“After two long drawn-out trials, which resulted in jury dismissals, the Indictments against Dr. William F. Koch and his brother, Louis charging them with marketing preparations falsely labeled as cures for cancer and other infections, was quashed today by Federal Judge Frank A. Picard.
“Dismissals of the Indictments, which was filed originally in April, 1942, was on a motion of Frank X. Norris, assistant United States attorney.
“In recommending the dismissals Norris said that the defendants, who did business as the Koch Laboratories, Inc., were now conforming with the Federal Food and Drug Laws in marketing their products.
“Norris said also he urged the dismissals because of the unusually long period of time that had been required for the two trials, the first of which ended in a disagreement by the jury. The second trial resulted in a dismissal, when one of the jurors became ill while the jury was deliberating on a verdict.
“The first trial started in January, 1943 before Judge Ernest A. O’Brien, and continued until May 28th of that year. The second trial ended July 23, 1946, after five months of Testimony. This trial was before Federal Judge Robert B. Nevin, of Cincinnati.”
Dr. Koch was about sixty-five miles from Detroit at a lakeside home working, writing, and vacationing. When his son heard the news, he drove all the way to where his father was staying, since there were no telephones there. What followed when he told Dr. Koch the news came to our attention more than six months afterwards through two secretaries who were working there at the time. Dr. Koch fell on his knees in the front room and thanked God for what had happened. When he arose, he prophetically made the remark: “While this is over, I feel that these people will never let me have peace. They will keep on working until they can find some other technicality to bring a new indictment. This will keep on until I am dead, for I have only a few more years left, at the most.”
GOVERNMENT INSPECTORS DISRUPT KOCH CLINIC ON A DAILY BASIS
The very next day the Food and Drug agents came to the Koch Laboratories, Inc., in Detroit, for a so-called “routine” inspection. They “inspected” every day for about three weeks, not even taking time off on Sundays or on Labor Day.
Dr. Koch was forced to come back from his much-needed rest. The agents wanted to watch every step and every detail of Koch’s laboratory procedures. Dr. Koch was willing to cooperate. However, he insisted on having technical and legal witnesses, whenever the agents were there. Soon the motives of these men became apparent. They had a stenographer take down their questions and answers. One of the agents went into a perfectly clean, sterilized room where air conditioning washed the air constantly. He went to a windowsill, wiped his finger across it, turned to his stenographer and placed into the record a remark that heavy dust was on the sill in the room where the laboratory work was done. One of Dr. Koch’s advisors, fortunately, did the same thing, held up his finger, and remarked, “There’s no dust here!” Dr. Koch used glass equipment, which had been sterilized under pressure. He would hold up a perfectly clean flask, pour some liquid into it, and after the liquid had started to enter the flask, the agent would ask something like this: “Tell me, Doctor, what kind of liquid was in that glass before you began to pour this into it?” The intimation being that the flask was not clean. Naturally after something is poured into it, there is no way of absolutely proving that it was clean and dry to begin with.
Dr. Koch is a man of integrity and honesty. This type of “investigation” irked him, and would any man who realized that the least slip might be the end. Here were his enemies trying to find a little straw, which they could grasp and turn into a new Indictment, possibly a charge of criminal negligence, or some such thing. The main point with the opposition is to stop the Treatment, regardless of the method used to accomplish this end.
DR. KOCH DECIDES TO STOP INTER-STATE COMMERCE
Before the investigation was completed to the satisfaction of the investigators, Dr. Koch came to the conclusion that the time had come for him to step out of inter-state commerce, and just keep up his private medical practice in Detroit. He knew that he was getting older and that this type of persecution would not cease. He was anxious to start letting up on much of his activity, since he was so in demand, that the call of duty nearly caused a collapse from the strain. Thousands of people are praying for Dr. Koch and the Koch Treatment every day. This wall of prayer has sealed him in and regardless of what happens, the cause for which he has given his entire time and life, will not die. A thousand seeds have taken root. The knowledge of the Koch Treatment is in the hands of too many people who in the struggle for victory over disease, will carry on the work regardless of what happens to Dr. Koch, the present laboratories, or the present workers.
Dr. Koch instructed his attorneys to write a letter to the Federal Government declaring in effect that as of a certain date in September, he was out of inter-state commerce and that the Koch Laboratories, Inc., were in the process of being dissolved as an organization. He also reminded the Federal Government that since he was no longer in inter-state commerce, it had no jurisdiction over his medical affairs relative to the intra-state commerce products. When the investigators came back on the day this letter took effect, Dr. Koch politely showed them the exit. The investigation stopped right then and there. Later, a physician who uses the Treatment in the Northwest told Dr. Reilly that Food and Drug agents had pestered him for three days, and had told him that Dr. Koch was uncooperative in the investigation last summer, and that Dr. Koch had “kicked” them out. The real truth is as it is stated here. They were trying to investigate something out of their jurisdiction. They say a man is “uncooperative,” because he is not willing to lie on the table and remain perfectly motionless while they stick pins and needles into his flesh.
The way these agents have hounded doctors, followed prescriptions of the Koch Remedies through the mails, threatened, intimidated, and attempted to make the doctors cease using the Treatment is not only un-American, but is decidedly the type of tactics used in Soviet Russia by communists. The public will come to know more and more about these methods and soon there will be a reaction that will eliminate these tyrannical, dictatorial, arrogant individuals from the Government. This is still a free country and men who represent the people should use fair and decent methods in treating those whom they suspect of violating the law, especially when it is so impossible to prove.
GOVERNMENT RELEASES CONFIDENTIAL INFORMATION TO THE PRESS
Information gained by these so-called “routine inspections” of a laboratory is considered confidential according to law. However, Food and Drug Attorney, William W. Goodrich, violated this law and turned over information gathered by Government authority, to Time magazine.
The Time article, couched in flippant phrases, contained this one damaging confession. It clearly showed that William Goodrich had given out information from Government files for smear purposes. Attorneys say that he is subject to prosecution for this action on his part, according to Section 301 of the Federal Food, Drug, and Cosmetic Act and General Regulations for its enforcement which provides:
“The following acts and the causing thereof are hereby prohibited:
“(j) The using by any person to his own advantages, or revealing, other than to the Administrator or officers of the Agency, or to the courts when relevant in any judicial proceeding under this Act, any information acquired under authority of section 405, 505, or 704 concerning any method of process which as a trade secret is entitled to protection.”
The policies of Time magazine must have changed considerably in the last fifteen years. On September 6, 1948 its medical columns were chosen by the opposition to inform the country that Dr. Koch is “probably the smartest, brightest quack in the U. S.” The idea behind this move was that one magazine with millions in circulation could with one article outdo all the good accomplished for the Treatment by Senator Langer and the religious publications which were behind it.
We know that Time editors received many, many letters protesting this article from people all over the nation, who were cured, if the letters received at Lutheran Research Society headquarters are any indication. Time, however, saw fit not to publish one single letter on the Koch side in its public letter column. Instead, a form letter was used to reply to these individuals. We know that prominent physicians and scientists wrote letters condemning the low type of smear tactics employed against Dr. Koch. Certainly these should have counted for something. Time printed none!
After Dr. Koch went out of inter-state commerce, the many physicians who depended on the Treatment to minister to their patients were left without a source of supply. Not only Dr. Koch’s office, but even the Lutheran Research Society’s office received visitors, long distance calls, telegrams, and letters from physicians in various parts of the nation who had patients dying for want of this Treatment. There was nothing that could be done.
For about one month progress was set back. Anyone who wanted the Koch Treatment was forced to come all the way to Detroit. The opposition made attempts, to get Dr. Koch to violate his promise that he was out of interstate commerce. They failed.
CHRISTIAN MEDICAL RESEARCH LEAGUE FOUNDED
Something had to be done. The ministerial friends who were constantly recommending the Treatment decided to see what could be accomplished. These many doctors had to be supplied.
After the blackout lasting approximately a month, an organization called Carbonyls, Inc., was established by a group of prominent men in Detroit, to manufacture the Koch Remedy. This was, at best, a temporary affair. At least physicians were once more supplied with the medicine they wanted and needed, but Dr. Koch was not a part of this new organization.
Dr. Koch often remarked to his ministerial friends that it was his desire to have his Treatment in the hands of Christian people before he died. These clergymen decided it was time to get busy if the work was to be preserved for humanity. A group of them gathered in Detroit, talked the matter over carefully with those concerned, and as a result, a non-profit corporation was formed. It is known as The Christian Medical Research League, Inc. On the Board of Directors are several clergymen of various persuasions, along with a few businessmen.
At the end of Thanksgiving Day in 1948, Dr. Koch left for Brazil and other parts of South America. Ever since 1942, he has been requested to come back there and complete work begun before the Government started to involve him in all this legal entanglement.
Persons close to the doctor wept silently when he boarded his plane at Willow Run Airport in Detroit. They wondered what would happen. As this is written and completed in March of 1949, Dr. Koch is still in South America, and does not expect to return to the states in the immediate future.
One medical doctor, who has used the Treatment for two decades, told one of the authors: “I would not blame Dr. Koch if he decided to stay in Brazil. The people down there treat him wonderfully, and he has scientific cooperation such as he never had in the United States.” Others, in Dr. Koch’s place, might well give such a thought serious consideration.
Without betraying confidences, and we pray Dr. Koch will forgive us, we would like to give you a few lines from a letter which the doctor wrote to a ministerial friend on Christmas Eve, 1948, from Brazil. Is really an “aside,” but will give the reader an insight into the type of God-fearing, Christ-centered man Dr. Koch really is in his every day life.
“December 24, 1948
“Dear Dr.,
“I presume you have written me lately, but as I was away from civilization I did not receive any news for a little while. However Dr…. comes today, I HOPE, with mail and some supplies. We will celebrate Christmas together.
“It is terrible to be away from the dear ones on Christmas. I wish I could be with you all. However, it seems from the best judgment I can use that this is the right place for me just now.
“For ten years I did not get more than three or four hours sleep out of a heavy day. Now I sleep from four p.m. on because I can’t stay awake and I often marvel how much a man can survive.
“We caught three big cobras yesterday, about five feet long, maybe the smallest was three feet. They are deadly poisonous, and live in the Garden of Eden. It is easy to catch them with a stick and a loop on the end that you can pull tight as soon as you slip it over his head when he is ready to strike. I do not like wandering in the jungle, but it is beautiful, and the flowers and fragrances are beyond words. There is peace here. The people are simple and kindly. They want to be good to you, and they succeed very well.”
“I shall send you a few pictures of the gigantic water falls under my balcony, and pictures of everything here in this mountainous jungle. It is cool day and night right in the tropics. No mosquitoes either. So far I have not run away from a tarantula as big as a cat, but they have them, they say, and sometimes they get into the house.
“Now it is Christmas morning, and torrents of cool rain are coming down. The mountains are hidden in the clouds and the rush of water down the falls shows that it is falling all around. I am working since 5:30 a.m. The work must be done as soon as possible, and then work kills loneliness.
“It is a lonely Christmas—all alone but for the Divine Presence and my thoughts.
Merry Christmas and a Wonderful New Year
Always yours,
“BILL”
This letter was much more lengthy, but we have merely quoted the human side of it to give an insight into the character of Dr. Koch: an extremely busy scientist, much in demand, working hard, helping people everywhere possible, a man of faith who even has time for the sentimental things which deal with life, family, and eternity.
Things were quiet in Detroit for several months after the Christian Medical Research League began to function. Dr. Koch was already in Brazil when it was officially organized.
This is truly the account of the birth pains of a new science. As one great European scientist wrote several years ago and many have repeated after him, “The Koch Treatment revolutionizes the entire field of medical thought. Science will come to it someday . . . it must come to it!”
What happens now to the Koch Treatment and the Koch Science depends on the public, on you, the individual. You can “have it. . . or you can lose it.” To have it you will have to protect it, fight for it. To lose it, you merely have to go on as before, and do nothing about it. Personally, we feel it is worth a real battle. It will either be a great boon to our generation, or God will continuously raise up men to protect it, and leave it for posterity.
At this point we wish to bring the history up to date in the present edition (1956) of this book. Therefore some of the material, which follows, is written several years after the previous material.
In the early part of 1949, agents of the Food and Drug Department made a routine inspection of the new laboratory used by the group, which is now entrusted with manufacturing the Koch Treatment.
It is to the credit of this group that they have spared no expense in setting up a laboratory, which is second to none of its kind as far as sterility, equipment, air-conditioning, etc., is concerned.
During the years since The Christian Medical Research League began to function, there has been no litigation on the part of the Federal Government agencies against the Treatment, except that in 1950, the Federal Trade Commission took action and declared the Temporary Injunction secured in 1942 a Permanent Injunction. The Judge who granted the Temporary Injunction at the request of AMA appeals had died in the meantime.
Doctor Koch is still in Brazil and is greatly engrossed in activity which will further the work so close to his heart. The writers who have attacked this book and Doctor Koch have made a great mystery intimating that he is hiding “somewhere in Brazil.” It takes several years to do research work and the doctor has been in Brazil almost eight years. Possibly he is completing such work in the near future. While in Brazil Dr. Koch, a widower for many years, married the widow of Rio’s most prominent physician, with whom he had worked years before. The new Mrs. Koch is a charming lady born in Austria, but who has lived in Rio for many years.
There have been individual attacks made by newspapers on local physicians who are using the Treatment. Generally speaking, these attacks have not done the harm, which they were intended. In one instance, which we know of, the physician became so much in demand after several smear articles in his local paper that he had to get an assistant doctor to help him take care of his practice. Needless to say, the newspaper in that city has stopped this tactic.
In past years there have been conventions of physicians using this Therapy to help each other in their work. Valuable papers have been given and the problems have been extremely worthwhile in attempting to answer many of the questions, which still need attention, and in acquainting new physicians with the methods of this Therapy.
Smaller regional conferences have been held in various parts of the United States with gratifying results in many instances.
There have been many attacks on the work since this book was first released, but they have only served as a guidepost of the progress that is being made.
Some magazines, newspapers, radio stations, and columnists have given the work excellent reporting, and for these we are grateful. There is more opportunity for small town editors to come to the front fearlessly in this matter than others, since they do not have the tremendous pressures hanging over them which large city-owned, chain newspapers have.
GOVERNMENT TURNS DOWN DR. KOCH’S OFFER TO CONDUCT TESTS IN A ‘PUBLIC’ FORUM
An offer was made by the manufacturing laboratory to the Food and Drug Department to carry on a public experiment with the Treatment where an equal number of Koch physicians could be in attendance with Government appointed doctors, and the entire results made public. The Government has declined the offer. We think it is a fair offer and if the Food and Drug were so certain that the Remedy is useless, they would have an opportunity of proving it for once and for all. Certainly “tests” made behind closed doors and in the analytical laboratory cannot be compared with honest, open, and public tests made in the clinic.
It is noteworthy that there are hundreds of more physicians who are using the Treatment in different parts of the country than there were a few years ago. Unfortunately, it requires the time of the doctor to really become acquainted with the technique before he can administer and observe the Treatment, properly. Wrong technique can spoil the entire work. This usually means a new physician who is interested must learn from more experienced physicians and must attend regional seminars, etc., in order to get this information.
In the intervening years, individual local attacks have been made on physicians using this method. Some of the doctors have won their cases and others are still pending. It is an indirect way of attempting to stifle the work, but, thank God, there are men of great courage in the medical profession who believe in truth above all else.
BENEDICT FITZGERALD, SPECIAL COUNSEL TO COMMITTEE ON INTERSTATE AND FOREIGN COMMERCE, ASKS FOR AN INVESTIGATION OF THE AMA
Hopeful signs were seen in the summer of 1953, when Benedict F. FitzGerald, Jr., Special Counsel to the Committee on Interstate and Foreign Commerce, issued a report to Senator John W. Brieker and members of the Committee, which has been described as the “most outstanding medical document in recent history.”
Mr. FitzGerald started his work under the late Senator Charles W. Tobey and at his request. Senator Tobey passed away before the report was finished, and Senator Bricker became the Chairman. For some reason, the report was never acted upon and Mr. FitzGerald was dismissed as Counsel.
The report was getting very close to the truth and it had a tremendous amount of pressure brought against it by the cancer fundraisers, such as the Damon Runyon Cancer Organization, The American Cancer Society, the drug trust, and others.
The report suggested a project, which would investigate the organizations, which have for so long impeded the progress of treatments under the AMA’s ban, and conduct research to see whether these blacklisted treatments did indeed have value.
Dr. Koch, and others, who have suffered under the whiplash of the AMA have long desired a Federal Government investigation, which would bring out the truth.
Whether some Congressman will have the courage to do something about the FitzGerald preliminary report on this subject, remains to be seen. At this writing, we have heard of such possibilities and our prayers are that they will materialize, Certainly Mr. FitzGerald, who is a prominent attorney, is a man of rare integrity, courage, and ability, and should have the support of all who feel the need for such investigations.
This is where the Koch Treatment stands today. It is known to many more thousands of people than ever before. It has gone through the birth pains and is trying to take its place in society. Its history is more dramatic than anything, which the mind of a Hollywood fiction writer could imagine. Now it is up to each person who has been helped by the Treatment to stand up and be counted for truth’s sake. If attacks come in the future, the public will not be unaware of it, as in the past, and thousands will come to the rescue and oppose these attacks. We request each reader to pray that there may be peace and that the opponents of the work will allow it to go on helping humanity.
IN THE FOLLOWING PAGES the reader will find that a considerable portion of the material is condensed from verbal Testimony given in court proceedings. As has been pointed out elsewhere, the written record of these proceedings runs into the thousands of pages.
The reader will observe, in many instances, a peculiar trait, especially where the direct quotations of a witness are used. Put yourself on the witness stand. Question after question is being asked. When put in writing from stenographic notes, the language is unpolished and jerky. The questions of the attorneys are not presented, so the authors have attempted to give the answers and statements of the witnesses in such a way that the question is apparent. This has saved considerable space and no essential evidence has been lost. This must be taken into consideration when reading this part of the book.
It is also essential to stress the fact that the task of attempting to reduce the photographic reproductions to a minimum was most laborious. Whenever references are made in the text to some X-ray, hospital record, or other document, which does not actually appear in the text, it is in the files of the publisher for confirmation. The verifying documents ran into dozens and dozens of pages occasionally just to establish a single case history. We have reproduced only a small fraction of what is available, in order to give the reader an inkling of the meticulous manner in which the material was prepared.
THE CASE OF CORA PRELL STERN
Introductory Remarks
THIS REPORT is intended to demonstrate that the Koch Treatment for tuberculosis does not follow the philosophy in practice throughout the world today, but rather is based upon the elimination of the germ’s pathogenicity by natural immunity induced in the patient. The current treatment of tuberculosis with cavities depends upon the closure of these cavities so they will empty their poisonous, infectious contents, and then perchance, the surfaces may heal together.
When cavities are larger than a third of an inch in diameter, and especially in large cavities, active measures must be taken surgically to close them. Pneumothorax, (that is, compressing the lung by letting air into the chest in the space between the surface of the lung and the chest wall to collapse the lung) is often successful. But adhesions may prevent such collapse. In such cases the phrenic nerve is cut to paralyze the diaphragm, (phrenicotomy) or the ribs are removed and pressure put on from the outside (thoracoplasty). Or the cavity, when thick-walled and large, may be drained through a tube to the outside (cavernostomy).
In severe cases where the other methods fail, the lung may be removed surgically (pulmonectomy or lobectomy). However, where the latter radical methods are employed, failure is the rule, for the patient is too far-gone to get well anyway, or is already surgically exhausted and in the vast majority of cases, the operation proves fatal. The shifting of the heart and many other changes that follow such procedures can prove fatal. At times the cavities are too large or their walls too thick to respond, or the disease is spread to the other lung and given impetus that hastens fatality. Thus the surgical approach is not too encouraging.
Conservative treatment (just bed rest) is not enough to secure collapse. Some active collapse method, as just mentioned, must be employed and it generally fails, too. Thus Barnes concludes in full agreement with other authorities (from a review of 1,454 cavity bearers) in his report in “The American Review of Tuberculosis,” 1928, Vol. 18, p. 412 that “statistics show the hopeless prognosis of cavitary tuberculosis conservatively treated.”
Likewise, Douglas, Saley, and Stringer state that, “it is probable that the majority of patients who are placed on bed rest alone will improve temporarily, but this very fact becomes a danger in that it leads to a false sense of security. Much time is saved and much risk is avoided by promptly augmenting bed rest with collapse therapy.”
To illustrate a cure of tuberculosis in the two especially dangerous classifications, we give the history of Cora Prell Stern. She started out with cavities in both lungs and the lesions were also, subapical. The significance of the former or bilateral type as reported by Barnes and Barnes in “The American Review of Tuberculosis,” 1935, “is 100% fatal, many of them not living over seven months.” The seriousness of the case with the subapical lesion, that is, located just below the level of the collar-bone, is well expressed in the words of Douglas and Pinner, “American Review of Tuberculosis,” 1935, “that the subapical lesion is of special clinical significance and develops with a more or less definite type of onset and rapidly progressive course, if untreated, has herewith additional support.”
Another serious aspect of the present case is that pneumothorax was attempted to collapse the cavities, but because of the pleural adhesions, turned out to be completely unsuccessful in the right lung and only partially successful in the left. The importance of completely collapsing the cavities by means of pneumothorax or otherwise is stated by Packard of the Trudeau Sanitarium in his text, “Artificial Pneumothorax,” p. 208. “An effective collapse is one in which the symptoms have subsided, the cavity can no longer be seen by X-ray, and tubercle bacilli have disappeared from the sputum on repeated examinations. As long as a cavity remains patent, or the sputum positive, the collapse is unsatisfactory and the patient’s chances for recovery are diminished. Statistical reviews have amply substantiated this statement.” By “cure” we mean the patient is free of all symptoms of the disease for a. period of more than five years.
Likewise, Pinner’s statement should be considered in judging this case, “Pulmonary Tuberculosis in the Adult,” p. 452. “In the hands of an experienced operator, it is rare that an effective pneumothorax can be established after several attempts have been unsuccessful.”
And, “finding tubercle bacilli in the sputum proves the activity of the lesion present and indicates need for treatment unless and until proved otherwise,” as stated by Douglas, Saley, and Stringer in “American Review of Tuberculosis,” Vol. 36, 1938.
In this patient the several negatives dominated the picture, a bilateral cavitation, subapical cavitation, and un-collapsible cavities. Her month spent between leaving the sanitarium and coming to the Koch Clinic brought a rapid decline, fever, blood streaked sputum, much tubercle germ laden sputum, and great weakness so that she would walk just about three or four hundred feet before collapsing. Her early status is presented from the Sunny Acres Hospital record and the radiograph shows the type of cavity on the right side. This is not a good photographic reproduction of the X-ray film, and does not show the condition of the left lung too well.
(Plate 2.)
The description of the last films taken at the Sanitarium is quoted from the Testimony of Dr. O. Hague, the expert who described them. He also describes what the X-ray taken after recovery shows and gives his estimate of the success of Treatment from the plates only. The best evidence, however, is offered in the patient’s Testimony, which is likewise reproduced. She made a rapid and full recovery, which appears to be permanent, after a dose of Glyoxylide. To satisfy her mind several other doses were also given at later dates. She is married and leads an active healthy life. Observers report in the spring of 1948, that she still remains free of the disease . . . fourteen years after Treatment.
It is quite evident in this case, therefore, and it will be observed in the others, that a dose of Glyoxylide may accomplish what both conservative treatment and active surgical treatment are not able to do; namely, get rid of the causative infection and to heal the cavities spontaneously. The attack is made on the cause of disease, therefore, and not simply on the products of the disease and then trust to luck for the cause to disappear. This type of Treatment is possible in the home and since too much bed rest is not required, a certain amount of work can be done while recovery is going on.
This is in sharp contrast to the rest treatment in vogue today, which only allows the patient a motionless whispering career under narcotics to suppress cough and other measures of enforced activity. When a patient on such a regime may improve to the point where he may be permitted to cut out pictures or write a letter he is supposed to be doing light manual labor, and if he should drive his car or do some other useful act he is doing heavy manual labor. While under active treatment and for long periods afterward, tuberculosis patients are carefully controlled. The advantage of a Treatment that permits the earning of a living and the support of the family while recovery is going on is, therefore, offering a great advantage to both patient and state from an economic standpoint.
TESTIMONY OF CORA PRELL STERN
(Note: the following is paraphrased from the Testimony given by Mrs. Cora Prell Stern at the Koch Trial and is found on pages 5837-5844 of the Official Court Record. The words below are those of Mrs. Stern.)
“My name is Cora Prell Stern and I live in Alpena, Michigan. It will be three years in June that I have lived there. I am married. I was not married when I first went to the Koch Clinic.
“In 1931 I was ill. I then lived in Cleveland, Ohio. I was very nervous and my hands trembled all the time. I also coughed and raised sputum. I went out to Dr. Crile’s Clinic in Cleveland where several of his physicians examined me. I had no treatment at that time. They recommended that I have a thyroid removed. That was a surgical operation.
“Following the operation I gained weight, but I did not feel much better. The trembling ceased some, but the coughing increased. This was still in 1931. I remained ill all during this time until 1932. During this time, tuberculosis had set in and I was coughing and raising sputum.
“When I left the Crile Clinic, they reported me to the Health Department and I went there for a checkup, in the tuberculosis unit. This was an outpatient department. Our office was being transferred at the time and I could not enter a sanitarium because everything was in turmoil and I was transferred to Detroit with the office.
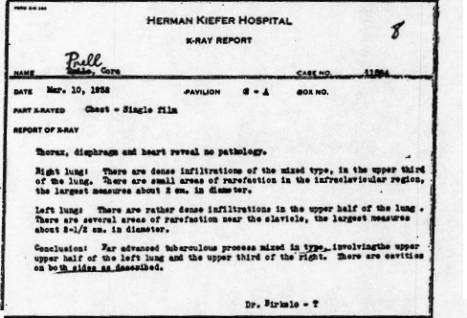
“About a month or six weeks after I arrived in Detroit, I came home one evening to find a letter in my box stating that if I did not come to Herman Kiefer Hospital for a check-up that they would send the police after me. I went. It frightened me, I assure you. “I went to Herman Kiefer and Dr. Durby talked with me and insisted that I come into the hospital. Not being a resident of Detroit, I naturally had to pay my way when I did enter. I entered in March 1932, (Plate 1) and had a Phrenectomy there. I do not recall the exact date. I was only there six months, so it probably was about three months after I entered.
PLATE 1. This is a copy of the hospital record in the case of Cora Prell Stern indicating, “far advanced tuberculous process.”
“I remained at Herman Kiefer for six months, but not having a residence there, I had to go back to Cleveland again. I ran out of money. I returned to Cleveland, to Sunny Acres Sanitarium, which is about fourteen miles out of Cleveland. It is at Warrensville, Ohio. When I returned to Cleveland from the Herman Kiefer Hospital, my condition was not improved. I had opened up another cavity, up in the right side. When I entered I only had it in the left; then I had it in the right. I did not feel any better. I was not up walking around. I was then in bed all the time and I coughed the same amount and was raising sputum and occasionally blood.
“When I entered Sunny Acres in Cleveland they tried pneumothorax on me. It was not very successful, but they did try it. I had too many adhesions though. Well, without any anesthetic they take a needle, which is a good size, and they just insert it right into your side between your ribs and then they put this air pressure in there as much as you can take or stand at the time and put you back in bed again. I do not know how many I had because I had them every ten days for the two years I was there. There were a great many. There was no improvement in my condition as a result of these treatments. I remained the same. I was there for two years.
“My aunt in Michigan was quite ill and I asked if I could come home to see her before she died. I asked the doctor at the sanitarium, the superintendent there, for permission. He said I could come, provided I returned to the sanitarium. I then went to see my aunt.
“At that time I had information about Dr. Koch. While I was in Detroit, I went to see him. I received a Treatment from Dr. Koch, which was administered by a hypodermic needle in the arm. The date of that Treatment was September 2nd, 1934. I noticed results from that Treatment. I went to work at my previous job on September 16th. I was doing clerical work at the railroad. I felt much better. The coughing stopped except when I would have a reaction. It would increase during the reaction and then it would retard and each time it would be less until I have not coughed now for years. I felt better almost immediately after the Treatment for I went back to work fourteen days later, on September 16th. (Note: this Testimony was given in 1946, twelve years after the Koch Treatment was administered.)
“It was approximately a month between the time I left Sunny Acres and the time of my first visit to Dr. Koch. I left Sunny Acres on August 4th and took my first Treatment from Dr. Koch on September 2nd, the same year. When I first visited Dr. Koch, I was very short of breath and was able to walk for a short distance only.”
TESTIMONY OF DR. OMER G. HAGUE
(Note: The following is a court-given description by Dr. Omer G. Hague, an expert radiologist, of a series of X-ray films made of Mrs. Cora Prell Stern when in public institutions before taking Koch Treatment.)
“This is a radiograph dated August, 1932, of a thorax of a female patient showing the breast cavities with a tuberculous process in the upper half of both lungs of an advanced degree with cavitations in the left apex, about three of them contiguous with one another, so I shall measure them all together. They measure two inches by one inch. That is the area covered by the three cavities. There are also some shadows in the opposite side that suggest smaller cavitations behind the second rib anteriorly on the right side. This area of whiteness is an extensive tuberculosis process in the upper lobe of the right lung.
“A similar condition exists on the left side, but it doesn’t show so much density as on the right because there is a cavitation process, which has taken away some of the fibrosis and that has been spat out as sputum.
“The descending bronchi are thickened because of repeated drainage from the upper areas of infection that have passed down into the lower bronchial trunks on both sides.
“The film dated November 5, 1932, shows the same patient with an aggravation of the disease in which there is a shadow in the right first inter space anteriorly suggesting cavitation, and an enlargement of the shadows on the left side indicating enlargement of the previous cavities. I believe an annular shadow that is on the left side in the previous film now shows that a reversible coupling has taken place at the C-10 meso position of the anthracene portion, leaving the next most reactive positions namely the C-4 and C-8 positions measuring three inches by two inches. I would say that this patient is worse on this film than on the previous one.
“In the film dated February 11, 1933, the tuberculous process in the right upper lung has increased. The cavitation is larger, measures an inch and a quarter outside measurements in both diameters. The total area of cavitation in the left upper lung is slightly more, but there is a concurrent factor of a pneumothorax in which there is air in the base and up over the upper lobe of that lung.
“What indicates the pneumothorax? The dark shadow with no signs of trabeculae in the area where there should be lung tissue.
“The lung is collapsed. You can see the border of the lung as a collapsed structure.
“In the upper area, the border is not so clearly defined because there are adhesions holding the cavitation to the rib wall and preventing a complete compression.
“Film dated May 17, 1933. The only significant change in these two sets of film is that there is a little better compression over the apex of this lung and one fairly strong adhesion band at a level of the third rib anteriorly is holding lung structure from complete collapse in that area.
“There is not much change in the appearance of the right lung, maybe a little bit more dense in its fibrosis.
“One would need to know the physical condition of the patient and breath sounds to state whether this was worse on this side, than the other one, and I have not that knowledge of the patient.
“The same conditions exist in the film dated August 16, 1933, with the exception that the outline of cavity in the right upper lobe, measuring two by one inches, is more clearly seen.
“There are still adhesions on the left side.
“It looks to me as if there were a little bit less collapse than on the previous film. It may be due to the fact that there is absorption of this air in the chest and that would make the variance.
“How often does air have to be put in during a pneumothorax? All patients are not alike. Some people need refills or larger amounts than others and oftener than others, depending on the rate that the blood absorbs the air and depending on the amount of air that is put in and any possible leakage. Sometimes it is done twice in a week and then it may be extended to once a week and then once every two or three weeks and that would be about an average, once in three to four weeks.
“Film taken November 29, 1933. I would say the left lung does not show any significant change from the left lung in the film immediately preceding, but the changes in the right upper lobe indicate the cavitation a little more sharply outlined and a little heavier in cavitation wall thickening which would suggest to me that there is more activity, and the response to the inflammation is characterized by a deposit of fibrous tissue surrounding that cavity. By ‘more cavity’ I mean the tuberculous process would be more active, creating more inflammation.
PLATE 2. This X-ray was taken on February 24, 1934 and shows the advance of tuberculosis after almost two year of hospital treatment in the case of Cora Prell Stern. See the Testimony of Dr. Omer C. Hague.
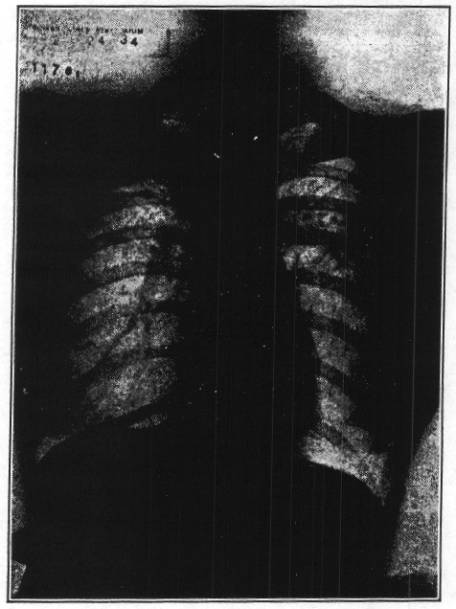
“This film taken February 24, 1934 (Plate No. 2) is a little lighter film than the one taken November 29, 1933. The right special cavity is clearly seen. The fibrous tissue surrounding it is a little less in density, but it is still present. (A film taken May 26, 1934, was then observed.)
“The last three views show no appreciable improvement under pneumothorax therapy. The diseased area of the left lung, with its cavitations, has not completely collapsed because there are adhesions remaining and the cavitation in the right apex with the associated fibrosis still exists and I would say that that is a very serious case of active tuberculosis.
“Assuming that this patient is still showing positive sputum at this time the prognosis in this patient is serious. They do not usually do well.
“From some observation of this set of films, it would appear to me that everything has been done that was reasonably possible by those who have had her in charge up to date.”
(Note: The former X-rays describe the condition before the patient received the Koch Treatment. The following were made after the Koch Treatment was administered.)
“The X-ray film dated February 18, 1942 (Plate 3) indicates a very marked improvement of this patient. The pneumothorax previously seen has now disappeared, the gas has been absorbed, and the lung has re-expanded to fill the chest cavity. The areas of former large cavities in this side, in the left upper first and second inter spaces, have practically gone and the annular shadow on the right side in the first inter space also is gone, but there still remains a mild fibrosis* in the first and second inter spaces at the site of the previous infection. There are fairly heavy hilar shadows in the left upper mediastinal area, which have come from inflammatory reaction of the large area of cavitation previously seen.
(*Fibrosis shows where healing has taken place.)
PLATE 3. This X-ray was taken on February 19, 1942 and shows the condition of Cora Prell Stern after the Koch Treatment. See the Testimony of Dr. Omer C. Hague.
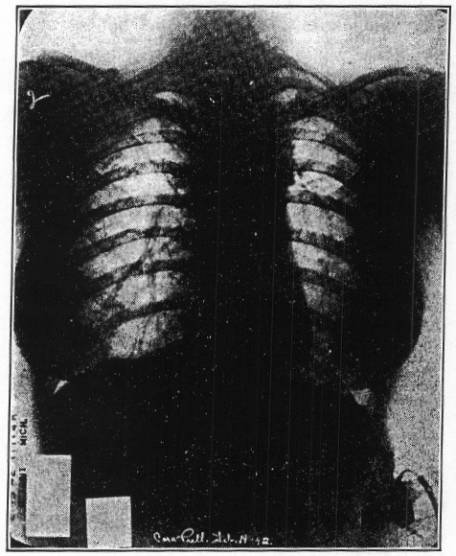
“The film taken March 22, 1943, does not show very much change from the one immediately preceding. I would say it is about stationary; the condition of the patient in this instance would be stationary with the condition in that one.
“Having seen all the cavitations of the left side and the large one on the right, these two films show a remarkable removal of disease process. It would he considered an excellent recovery if it were in the ordinary course of observation in a sanitarium. We would consider that a cure, under sanitarium conditions.”
AN ANALYSIS OF THE REBUTTAL OF THE CORA PRELL STERN CASE ATTEMPTED BY DR. BRUCE DOUGLAS
On page 7367 in the Court Record, Dr. Douglas testifies that the removal of the thyroid lessened the aggravation of the tuberculosis. This along with treatment and rest cured the patient. On page 7955, he testifies that this case considered totally was far advanced on February 24, 1934, when she left the sanitarium.
On cross-examination Dr. Douglas testifies on page, 7987, 7990, and 7999, that the pneumothorax treatment she had received for two years in the institution was not effective and that some new method of treatment should he employed — some additional collapse therapy. In other words, Dr. Douglas testified that the disease was still progressive and something additional had to be done. However, as Goldberg states on page B140 of his text, “Clinical Tuberculosis,” Vol. 1, “Collapsed therapy is done only for the closure of cavities. It has little or no effect on the chronic productive tuberculosis which spreads as it pleases in the collapsed lung.”
The history given by this patient and Dr. Koch, shows the exhausted condition and extensive flare-up she was suffering at the time she received his Treatment. The effort she had made on leaving the institution was too much for her and a serious breakdown in her resistance and relapse took place, making the disease far worse than the data showed that was available at the institution when she left.
It was evident that the Treatment she received was far better than the additional collapse therapy Dr. Douglas recommended as necessary, since the lung was preserved and permitted to heal as the disease was eliminated.
Recovery was rapid also. She was back to work in a few weeks. Further collapse therapy with or without Thoracoplasty would have required years of bed rest and even then as Goldberg points out the disease might still progress. Indeed, years of the best institutional care with collapse therapy already had failed to halt its progress, in this case thus showing the collapse therapy was futile.
Pulmonary Tuberculosis
THE CASE OF STANLEY MOSEVICH
Introductory Remarks
The following case also demonstrates the recovery of far advanced tuberculosis with an enormous cavity with thick walls and located close to the mediastinum, (near the heart). In fact, the medial wall merges with the enlarged glands of the mediastinum. Such a cavity is not amenable to any form of collapse therapy whatsoever, even the most radical measures such as cavernostomy or lobectomy removing the lung.
As stated in the hospital record, it is a case of far advanced tuberculosis permanently and completely disabling the patient. He was examined at the Herman Kiefer Hospital, the diagnosis was made, but no attempt was made at treatment. Instead he was encouraged to go to the Koch Clinic where he received Treatment with Glyoxylide, which was followed by full recovery. If the X-rays taken before and after Treatment are compared, it will be seen that the disease tissue has been completely cleaned out and replaced by normal lung tissue. His sputum became negative to tubercle bacilli before the large cavitation was completely healed. Thus the recovery depended upon the destruction of the causative agent and not upon the drainage of the cavity.
This was a retention cavity. The fluid level at the bottom shows that it did not empty. It was the type of cavity where one wall, the upper wall, was ulcerated out. In other words, the defense wall had broken down and the infection had spread widely throughout both lungs. In fact, the military* seeding of the lung parenchyma (functioning tissue) with the many small caseous tubercles, some of which are coalescing to form large caseous deposits, gives the picture of an established military tuberculosis in both lungs, and especially in the lower lobe of the left lung. The X-ray films taken at the Herman Kiefer Hospital and at the Koch Clinic both show this change.
(* Military means “galloping consumption” -very widespread.)
It is to be noted that this patient was not placed on strict bed rest but was allowed to do as he pleased, taking a few hours’ rest each afternoon, but he did his own cooking, shopping, and drove his car about sixty miles through the heavy traffic of the City of Detroit every two weeks to visit the Koch Clinic. This was, indeed, hard manual labor for a man in this condition.
One should contrast this type of Treatment with the enforced absolute bed rest required of tuberculosis patients who though having much less infection and lung destruction must practice perfect immobilization and learn to relax their muscles and keep them inactive, and not even speak above a whisper. Thus the recovery was secured after the Koch Therapy, while following entirely different procedure. The fundamental principle of raising the natural oxidative resistance to infection in the body so high that even under the unfavorable circumstances recognized by regular methods, recovery becomes possible, which was the goal.
Dr. Koch’s Court Testimony, together with descriptions of the X-ray films given by the radiologists of the Herman Kiefer Hospital are followed by the report of Dr. Hague.
DR. KOCH’S COURT TESTIMONY
“Mr. Mosevich came to me on October 20th, 1938, with a history of a father who died of intestinal obstruction. His previous illnesses were pneumonia in 1935, pleurisy before the pneumonia set in, and the pleurisy was in the left chest.
“In September, 1938, he began feeling badly; he began coughing and arising; had night sweats.
“He went to the Herman Kiefer Hospital for X-ray pictures and the diagnosis of tuberculosis was made (far advanced, permanently disabled.)
“We took his sputum and sent it into the Michigan State Board of Health for a report and we ran our own tests too, and the sputum showed tuberculosis. We received the report from the Board of Health that it was positive and we confirmed it.
“We also made an X-ray picture of the chest which showed a huge cavity in the left lung located at the root of the lung, that is, at the hilar region.
“The bottom of the cavity shows a horizontal line straight across, which is a fluid level showing that this cavity contained fluid. It belongs to the class of cavities called retention cavities and that fact gives it a very important significance.
“Retention cavity is one that leads into a bronchus that is closed or stenosed — closed down so tightly that the contents cannot escape — that is, escape completely. Of course, some debris remaining in that cavity which is always being absorbed gets out. But, there is a certain amount of infection and tissue and poisoning the individual, and which is the source for spread of the infection through the rest of the system.
“That shows that the cavity is not the type which collapses readily. In order to collapse naturally, the contents of the cavity must be eliminated, squeezed out, whether it is air or pus or whatever the material may be. And a retention cavity does not close; it remains open, because of tension, the pressure on the inside is greater than the outside. The procedure for handling such cavities is to remove the lung or to cut a hole through the lung, through the cavity wall, to secure drainage and to help collapse it. However, with a thick wall, collapse is not possible in this position.
“I made a diagnosis of far advanced tuberculosis of the lungs.
“I gave him a Treatment of Glyoxylide on October 24th, 1938, at which time his weight was 153.5 pounds, his normal weight being 182 pounds.
“The hospital record contains the following letters:
“Dear Doctor:
“With reference to the above named I wish to advise that our X-ray examination of 9-16-38 revealed as follows:
“Diaphragm: The costophrenic angle on the left is obliterated. The heart is normal. Right lung: There is a small amount of fibrosis visible in the infra-clavicular region. No other abnormality is found. Left lung: There is considerable mottling throughout the lower 2/3 of the lung with a large excavation near the root, measuring about 7 cn. in diameter and showing a definite fluid level. Sputum examinations have been reported as positive for tubercle bacilli.
“Hospitalization has been recommended. If this meets with your approval kindly let us hear from you in order that the necessary arrangements can be made.
“Yours very truly,
“A. P. Derby, M. D.
“Director, Out-Patient Dept.”
“March 10, 1939.
“Chrysler Industrial Association,
“7900 Jos. Campau Avenue,
“Detroit, Michigan.
“Dear Dr. Mosevich:
“In re: Stanley Mosevich
“Stanley Mosevich was examined here on July 19th and I have procured the films from Dr. West for comparison.
“This man has a far advanced pulmonary tuberculosis and while there has been some clinical improvement since last September, still there is evidence of quite extensive disease of both lungs and sputum, tests run last month in the laboratory here showed the sputum to be strongly positive for tubercle bacilli. With a disease of this extent existing for this length of time it would be my opinion that this man is totally and permanently disabled because of pulmonary tuberculosis.
“Yours very truly,
“Bruce H. Douglas, M. D.
“Tuberculosis Controller.”
“Film No. 2 was taken July 8th, 1939. That is less than a year after Film No. 1 was made.
“In Film No. 2 you do not see the cavity as such any more. However, the tubercular scattering through the lung, which is observed in Film No. 1, is observed in these little speckles throughout the field, and also in the right lung there is some indication of the spread of myriads of small lesions of tuberculosis.
“They are very definite in the left lung. In fact, below the large cavity there is an accumulation of tubercles, forming an agglomerate an inch in diameter which looks as though they might break down to form another cavity, if they had time to do so. However, in Film No. 2, which was taken almost, a year after Film No. 1, the large cavity does not show and there are favorable changes going on in these scattered lesions of tuberculosis.
“The changes indicate improvement. This type of change we observe in our films quite frequently, in that the lesions become vascularized, and they show these soft densities. Moreover, the agglomerate of small tubercles, that formed a fairly large mass below the cavity, has lost its individuality. It is being absorbed and is disappearing as seen in the third film.
“In Film No. 3 one can easily see that the lung is clear; there is no sign of a cavity left. This film is dated June 18th, 1940.”
During this time, he was doing what is considered hard manual labor for a tuberculosis patient. He went to the Dodge Motor Plant to work in 1942 and Dr. Ford, the factory radiologist, made X-ray films during the health examination for admission. These showed complete recovery and his ability to do hard manual labor, not only at regular hours but overtime as well. The Government did not ask Dr. Ford to testify, but the films were admitted and showed Mosevich was cured. He worked as a metal polisher for several years, and then in a brewery a number of years, where he carried heavy casks of beer. He remains in perfect health and was so reported on June 4, 1946. Another thing that is important, under ordinary treatment this man would be kept absolutely bedfast: he would not be allowed to turn in bed, hardly. Under the Koch Treatment, he was not restricted except being told to use common sense and not let himself get tired. And it was not very long afterwards that he was moving around as he pleased and was working within a couple of years (1942).
A matter of interest can be found in two Photostats in the publisher’s files. They show that the Department of Health sent this hopeless Mosevich case to Dr. Koch and immediately notified the Police Division, Major Roehi, about it. This was to watch the patient come to an early death, as such cases regularly do in their experience. As soon as Mosevich should pass on, we suspect Koch was to be arrested on some sort of frame-up. However, Mosevich got well rapidly and stayed well.
COURT TESTIMONY OF DR. OMER GRENVILLE HAGUE DESCRIBING THE X-RAY FILMS ON THE STANLEY MOSEVICH CASE
“The radiograph of September 16, 1938, is that of a male chest with the bony cage and ribs and collarbones and heart shadow in the middle and diaphragm down here. There are some infiltration shadows in the parenchyma, or the active portion of the lung in these areas, in the fourth, fifth, sixth, and seventh, inter spaces anteriorly and a large cavitation shadow in the mid-lung zone. I am measuring the left lung. That cavity measures 2.5 inches by 31% inches, a little better than 31/4 inches. The outside measurement of the capsule of the cavity.
“By a little better than 3 1/4 inches I mean about 1/2 an inch more. The reason I am not saying that with certitude is that the upper border of that cavity is very, very thin and very, very faint, but we can see the line that it follows and I would say it would be 3 1/4 inches at least. That is being very conservative.
“There is a small fluid level at the bottom of that cavity. There are, also, some heavy hilar shadows, and some thickening of the peribronchial trunks; that is, the lymphatics that follow the bronchi and smaller bronchioles. Those shadows indicate repeated infections that have resulted in inflammation and the inflammation has gone on scarring.
“The film dated July 8th, 1939, appears to he a film of the same chest; the ribs strip with the previous film. The lung tissues on both sides show soft infiltrated shadows throughout the lower two-thirds of both lungs.
“There is an interlobar line, indicating a thickening of the pleura between the middle and lower lobes, on the right side. There is a shadow in this area. It is smaller than the cavity on the left side previously referred to. It is in the same inter space level, so that I conclude it is related to the previous cavity. It measures 1.5 inches by 1 inch. The wall of this cavity is less distinct. That is why it is a little harder to see. The shadows in the lung are of a soft consistency, which would suggest an activity of disease in the lung structure itself.
“In the film dated September 16th, 1938, the linear markings are fairly well fibrosed, hard. In the film dated July 8th, 1939, we see them softened and in an active state of inflammatory change. In the film dated June 18th, 1940, this inflammatory reaction has disappeared and the outline of the cavity is very, very faint, practically disappeared. It would be about one inch by an inch and a quarter. The general appearance of this chest is much better than in the films taken September 16th, 1938, and July 8th, 1939.
“Cavities almost of any size are a poor prognosis type of tuberculosis cases. The tendency usually is that individuals who have cavitation develop more cavitations rather than less. Cavities usually tend to get larger and unless they are treated successfully by a pneumothorax, or some other compression therapy, and are held down for a long time, they usually get worse and the patient’s outlook is serious.
“The cavity in the film dated September 16th, 1938, I think is about as large a one as I have ever seen and I would say that that patient’s condition would not be a good risk at all.
“The two succeeding pictures dated July 8th, 1939, and July 18th, 1940, show that there has been an extensive constitutional change taking place; that is, the soft tissue of the lung has undergone a remarkable exudative change; that is, there is a softening of the structure all through and in an instance like this that patient would have more cough and more sputum and it might be in the healing phase following this type of a chest. For instance, the tubercle from this cavity may have been coughed up and spread out throughout the whole lung and that might be a cause for the infection from here to become broad spread in that chest almost like a tuberculous pneumonic condition and then in this view, Film No. 3, this pneumonic process has disappeared and the shadows in the lung are back to what you would expect of an individual of this age and following conditions of a tuberculous recovery.
“The prognosis on the first film dated September 16th, 1938, would indicate a very serious situation.
“The prognosis on the third film dated June 18th, 1940, without knowing anything about the other two, would be very good.”
THE TESTIMONY OF STANLEY MOSEVICH
(Note: The following is paraphrased from the Court Testimony of Stanley Mosevich, pages, 7516-7538.)
“My name is Stanley Mosevich and I live in Detroit, Michigan. I am employed as a metal finisher in the Fisher Body Plant. In 1938 I went to see Dr. Podezwa in Hamtramack, Michigan. He sent me to the Herman Kiefer Hospital where a diagnosis of far advanced tuberculosis was made. No treatment was given me there since they decided my case was too far advanced to get well. I, therefore, chose to go to the Koch Clinic and the doctors at the hospital thought it was a good idea.
“My symptoms were that I was sweating at night very profusely and I was coughing up blood and pus. I had become quite weak from all this and there was some pain in the left side and in the back between the shoulder blades. This started in July 1938, and was very annoying by September. The Board of Health and Herman Kiefer Hospital found my sputum to contain the tubercle germs.
“I took Dr. Koch’s Treatment. After that I had some reactions, times during which I felt feverish and coughed more than usual, but after each reaction, I improved and finally the reactions were so light, they were scarcely noticeable. This was at about October 1939, and after that there were no more reactions to be noticed. I had gained weight, going up from 153 to 204 pounds by this time, which was just a year after I received Dr. Koch’s Treatment.
“My strength improved in the same way, too. In fact, I did not let myself get too weak by lying in bed too much. I did as Dr. Koch directed me; that is, not to get too tired, but to be up and about some, taking rest when I felt I needed it. So I got up early in the morning, about seven o’clock and stayed up until afternoon when I took a few hours rest in bed.
“Then I got up for supper and went to bed at nine in the evening or later, I also went about and did the shopping and the cooking and I drove to Dr. Koch’s office through all the Detroit traffic every week or two and back to the country, a total distance of about sixty miles or perhaps more. I stayed in the country about two years and then returned to Detroit where I finished my recovery.
“In 1942 I took a job at the Dodge Auto Factory and worked overtime as a metal polisher for a long time. This is heavy work. I thrived on it, too. Recently I have been working at carrying and piling up kegs of beer and more recently I have been carrying large heavy pieces of plate glass.
“My health is perfect and has been since about two years after taking the Koch Treatment. If I ever get tuberculosis again I want Dr. Koch’s Treatment.”
(Note: This latter Testimony was given in the 1946 Trial.)
AN ANALYSIS OF THE REBUTTAL OF THE STANLEY MOSEVICH CASE ATTEMPTED BY DR. BRUCE DOUGLAS
The rebuttal was offered by Dr. Douglas who stated on direct examination for the Government on page 7869 and 7877, “The improvement was entirely compatible with what might be the course of a case of tuberculosis of this extent under a moderate rest program, while not working.” Contrast with this statement required by the Government, the statement made by Dr. Douglas when Mosevich was examined by him and only a health problem was at stake, thus from page 14 of the hospital record we read: “This man is totally and permanently disabled because of pulmonary tuberculosis.” Also contrast with it the statement made by Dr. Douglas on cross-examination appearing on page 8006 and 8049, that “pneumothorax for two years at a minimum which would have to be continued more or less indefinitely would be required on the treatment of this patient.”
Even in this statement the ultimate prognosis of fatality is suggested. It is evident that the Koch Treatment which Mosevich received proved far superior to the treatment just suggested and rescued Mosevich from the condition described in the hospital record as hopeless and permanent.
The enforced bed rest which is always required of such patients involving complete relaxation of the muscles, restriction of breathing to the most shallow that can be sustained, the prohibition of talking above a whisper, bedpan service, etc., and if the patient is permitted to do light manual labor, it is merely the writing of a short letter, intermittent periods of reading, or cutting out pictures while the patient is lying flat in bed, or the exercise of being wheeled in the chair to the bathroom and back, or the eating of a meal while sitting up, must be compared with the work which Mosevich carried on from the start of his Treatment which involved doing the chores about the house, cooking, going shopping, and driving his car some 30 miles each way across dense traffic of Detroit every week or two as he testified, in comparison, these acts are heavy manual labor and are sufficient to tire many healthy people who do not have tuberculosis. So, Dr. Douglas’ Direct Testimony in rebuttal does not apply in this case as the facts reveal, but he is forced to admit on cross examination as reluctantly as he could, the truth of what he stated in 1939 when he first examined the patient — “This man is totally and permanently disabled because of Pulmonary Tuberculosis.”
Pulmonary Tuberculosis
THE CASE OF STANLEY SANCHEZ
Introductory Remarks
The case of Stanley Sanchez is one in which modern tuberculosis surgery went the limit without success. For five years, from June 1929, to March 1934, he was under the most expert care that modern institutions can offer and yet with all the sacrifice and suffering nothing was gained. He steadily became worse. Strict bed rest and collapse therapy including many pneumothorax attempts and complete left side thoracoplasty (removal of his ribs) done in three stages could not close the cavitation. The sputum was copious, positive to the tubercle bacillus and occasional serious hemorrhages took place, plus a good deal of streaking in between. Finally after five years of this it was decided by the staff of the municipal tuberculosis hospitals of Detroit in conference on his case that further surgery was required. (Plate 4)
All that could be left for surgery to attempt would be a revision operation or a pulmonectomy, the removal of the lung surgically and that could not be done because of the great number of adhesions that had formed between the lung and chest wall and because of the already bad position of the heart and mediastinal structures. These attempts would be grasping at straws, indeed.
In order to make plain the position of the patient at this time it would be well to review the statements of authoritative writers on the subject. Thus Julius L. Wilson, Med. Ulin. No. Amer. 29: 445 (March) 1945, Selected Writings, Ochsner Clinic, New Orleans, June 30, 1945, Vol. IV, P. 43 and 44, states:
“Pulmonary Resection—The second method of treating the tension cavity resisting other forms of therapy is pulmonary resection. Since lobectomy or even pneumonectomy of a non-adherent lung is a simpler operation than a two or three stage thoracoplasty, there is a temptation to substitute one of these radical methods of resection for the other measures of collapse therapy. However, pulmonary tuberculosis in the stages severe enough to require major surgical procedures is seldom confined to one lobe or even to one lung and, of course, the lesion here is only a manifestation of a generalized disease.”
Pinner, p. 467, states:
“After unsuccessful thoracoplasty, revision operations have been attempted but are very dangerous. Many of these patients run the entire gamut of all possible collapse measures, ending usually with an unsuccessful thoracoplasty. At this point, patient and physician face the various modifications of ‘revision’ operations, such as anterior costectomy and resection of the regenerated ribs. These operations, particularly the latter, are technically difficult and their danger is potentiated because they are performed on ‘surgically exhausted patients.’ The rate of success of revision operations is small in most published series and probably still smaller in unpublished work. The operative mortality is relatively high.”
In the Sanchez Case, the infection had gone beyond the chest confines moreover, as Wilson explained above, and in this case it had produced a rectal fistula, a branching abscess caused by the tubercle bacillus, which emptied into the rectum. It was operated, but not successfully and he still carried this infection when he was taken to Dr. Koch for Treatment, as Dr. Koch’s Testimony showed. Up to this time, the only activity he had was to be wheeled to the bathroom and back to bed. Otherwise, he was on strict bed rest.
FROM DR. KOCH’S TESTIMONY WE TAKE THE FOLLOWING DATA
His color was sallow, very anemic, somewhat cyanosed and the heartbeat was very rapid and weak and the respirations were quick and labored. He was coughing a great deal and raising quantities of tubercle-laden sputum and appeared quite exhausted even in bed. He could not walk without help. On March 26th, 1934, his weight was 117 pounds, he claimed. His first injection of Glyoxylide was given on April 3rd. 1934. Other injections were made each year to insure the permanency of his recovery, whether needed or not.
The recovery was quite rapid in that the sputum became negative in about four months and except for the reaction periods there was very little or no sputum at all after that. At his fifteenth week reaction there was a copious hemorrhage. After that the recovery was more rapid. He was soon engaged in heavy manual labor at which he continues to date.
From the large hospital record a few pertinent statements are extracted and the final sheet is also reproduced where it states, “February 26th, 1934, — conference voted to refer to surgeon for further surgical collapse of left lung.” This was just before he was taken to Dr. Koch and shows he was desperately in need of help. (Plate 4)
PLATE 4. This is one of the sanitarium records in the Case of Stanley Sanchez. Note particularly the last entry, “February 26, 1934 Conference voted to refer to surgeon for further surgical collapse of left lung.”
From the hospital record of the Herman Kiefer Hospital, Tuberculosis Division, dated June 23rd, 1929, the following statements are taken.
The diagnosis: “Admission — pulmonary tuberculosis.”
Add the figures, “VII—B.”
Under date of November 4th, 1930, Case No. 8006, under the caption, “Interval History:” “Patient was transferred to Maybury on November 3rd, 1929. Artificial pneumothorax was instituted prior to his discharge from here. At Maybury patient had several small hemorrhages. Also developed effusion. Was transferred here for thoracoplasty.”
The operative procedure, August 29th, 1929: “One inch incision posterior border sternocleido; scalenus exposed by blunt dissection. Phrenic bound crossing the outer border of the scalenus. It was injected, severed and 17 centimeters removed. Wound closed with two skin clips.”
Second operation, November 7, 1930: Surgeon: D. O’Brien; Assistant: Dr. Brown; Assistant: Dr. Lullock; Surgical Nurse: Miss McCarty. Started the operation at 8:50 a. m.; finished it at 9:10 a.m. “Clinical diagnosis: Pulmonary tuberculosis. Left first lower stage thoracoplasty. “Operative Procedure: 10 inch incision paravertebral; thoracic cage exposed. Sections of the 8th, 9th, 10th, and 11th ribs removed subperiostally. About 10 centimeters of each removed. Posterior stumps removed with Sauerbruch. Wound closed without drainage. No complications.
This operation, November 28, 1930: Surgeon: O ‘Brien; Assistant: Klein; Assistant: Lullock. Surgical Nurse: McCarty. The time of the operation, started at 9:00 a.m., finished, 9:21 a.m. “Clinical Diagnosis: Pulmonary tuberculosis. Left second stage thoracoplasty.” “Operative Procedure: 10 inch incision paravertebral; thoracic cage exposed. It was necessary to make about 3 inch transverse incision at the middle of the wound. About 14 centimeters of the fourth, fifth, and sixth ribs, removed superiostally. Posterior stumps removed with Sauerbruch. Wound closed without drainage. No complications.”
From the same hospital record: still another permission for operation, Estanislao Sanchez, third-stage thoracoplasty. And under date of December 19th, 1930, the same patient, Estanislao Sanchez, Case No. 8006, the same surgeon, O’Brien; Assistant, Brown; Assistant, Lullock; Surgical Nurse appears to be McCarty and Connor. Time that the operation started, 10:00 a.m., time finished 10:35 a.m. Clinical Diagnosis: Pulmonary Tuberculosis. Third upper stage thoracoplasty. “Operative Procedure: 12 inch incision paravertebral, thoracic cage exposed. 1.4 centimeters of the second and third ribs, and 8 centimeters of the first, removed superiostally. No complications. Wound closed without drainage.”
From the same hospital record: still another permission for operation, signed by a member of the Sanchez family, the same Case No. 8006, under date of June 30th, 1931. This time the surgeon is Dr. Corbett. Assistant doctor, Lullock. Clinical diagnosis is: Rectal fistula, probably tuberculous. Fistulectomy. “Operative Procedure: Two fistulous openings were found posterior and to the left of the external sphincter. These were found to communicate with a large undermined area external to the external sphincter. Fistulous tract was found to communicate with the rectum immediately about the internal sphincter. The entire fistulous tract was laid open and cauterized with the actual cautery. One iodoform was inserted.” This shows that the disease had spread beyond the chest to other parts of the body, and was not under control.
THE TESTIMONY OF STANLEY SANCHEZ
“My name is Estanislao Sanchez. I am better known as Stanley. I live in Detroit, Michigan. I am a gasoline station attendant. I am a tune-up man. I overhaul generators, starters, distributors, anything about an automobile, such as brake checks, taking mufflers off and putting new ones on, greasing automobiles, selling gas, anything in the line of the automobile.
No internal stuff such as rings or valves; we do not do that as we do not have the time or space.
“I work under all kinds of conditions. We have no heating in this garage. It is damp and in the wintertime it does get kind of chilly and in the summertime when we tune up an automobile, we use caseite, we make a lot of smoke and fumes and that is kind of bad.
“I was ill in 1928. I thought I had a severe cold. I had chills and a cough and I was feeling bad all around. I consulted medical advice and was examined and X-rayed and the doctor here said that I was sick, that I had a contagious disease or something; anyway my dad, at the time took me down to Texas.
“Another doctor gave me some kind of shots to keep me going for a while. I was down in Texas several times on short visits. I was down there the first time about a month and then I was there about three different times. I cannot tell you exactly how long each time, but I was back in Detroit in June 1929.
“The state of my health then was bad. I was out playing baseball and I had a bad hemorrhage from the lung. We called a doctor and I was told that I was supposed to go to Herman Kiefer Hospital.
“I went there and they started giving me some pneumothorax; they put a needle in between my ribs and pumped some gas, or something, into me to collapse the lung. I remained at Herman Kiefer Hospital at that time about three to four months.
“Just before I left Herman Kiefer they gave me a phrenectomy, an operation at the neck, and I do not know what they did; all I know is they were supposed to pull a nerve, or something, up to lift my lung up, and then they sent me to Northville, to the Maybury Sanitarium. That is about 30 miles from Detroit.
“I went directly there and my condition did not improve at Maybury Sanitarium. I went to the Maybury Sanitarium in October or November and stayed there just about a year.
“I received pneumothorax treatments there. My condition did not improve while I was there. I became weaker. I stayed at Maybury Sanitarium for about a year.
“They then sent me back to Herman Kiefer Hospital in Detroit. I received my first stage of thoracoplasty there, about a week or two after I had been back from Northville. This thoracoplasty was an operation on my back and naturally I cannot see on my back, but they operated on my back and they removed some ribs, so they said, anyway. When they finished with me, I was taped with adhesive tape underneath and then they had a binder over me. They kept me like that for several days and the worst part of it was about a week and it was rather a painful affair, as I believe anybody that has an operation where a bone is involved would testify. I was confined to my bed following that operation. I could not move around.
“They had me on the top of the side I was operated and I was supposed to lie on it with pillows under my back holding me without moving one way or the other.
“I did not have a chance to notice any result of that first thoracoplasty. Three weeks later they had me up again for another one. I had a second thoracoplasty just going right through the same procedure as it did on the first one; everything went on the same; what I mean by that is, I was in bed, and I went through the same thing with my second as I did with my first.
“I did not notice any results from the second thoracoplasty. I was still in the same position when I got my third operation. I had a third thoracoplasty, the same thing as the other two.
“It was several months before they let me sit up in bed and I was rather thin, weak; did not gain much weight. I was still coughing, raising a very little. Right after the operation I was not raising any blood. I started raising blood after while. I would say after about three or four months I started streaking. When I was streaking, I would call that a little bit of blood on the sputum.
“I was in Herman Kiefer Hospital on that occasion, for the series of operations, for about eight months. I weighed about 117 pounds at that time.
“I was then sent back to Maybury Sanitarium at Northville. That would be in 1931. I was put in bed and kept right in bed until I left. I was still coughing. I certainly did hemorrhage. At that time I remained in Maybury Sanitarium about two years and seven months. Altogether, it was four years and nine months, during the stretch; Herman Kiefer, Northville, back and forth; but that last one was about two years and eight months, something like that at Maybury Sanitarium.
“At the end of that time at Maybury, I observed that I was getting nowhere. I was flat in bed. I was not gaining any weight; I was coughing, hemorrhaging. Every time I would raise sputum it would be clouded with blood. All in all, I was not getting any place. I was in bed and I weighed 122 pounds.
“After I had been there for that time they were going to give me another operation under the apex or under the arm. I had already written a letter to Dr. Koch. I had heard about him, so I figured I would go home and take a chance with Dr. Koch’s Treatment rather than another operation.
“I went to see Dr. Koch and received a Treatment from him on April 2nd, 1934. I started feeling better. About five weeks after I received Dr. Koch’s Treatment, I was able to walk around a little, not too much, but I was able to walk around. I observed other results. On reaction weeks I really felt bad. I had heard about reaction weeks. I did not experience it up to this, but I was feeling perfectly all right. In fact, I was feeling extra good. I started getting a headache and at the time I was home, so the next thing to do was to go back to bed because I had heard that it was supposed to be a reaction. Then I started getting a temperature. One minute I would feel hot and the next minute I would feel cold. I had about six blankets on me and a hot water bottle on my feet. This lasted for about two or three hours. One week it would affect me one way and the next it would be different. Sometimes it would affect me two or three hours. I was weak and would have a temperature. It would go up to about 103 degrees and I would cough and raise a lot, but after the reaction I would feel better than before I had gotten sick. During the reaction there was evidence of blood in the raising of the phlegm or sputum.
“I would say I had my last hemorrhage after I had been with Dr. Koch for about a year, but I raised blood in the sputum for about a year and a half after I was with him.
“I had a second Koch Treatment during my fifteenth and sixteenth week. I could not tell you the exact date, but it was during the fifteenth and sixteenth week. I had a hemorrhage and the doctor thought it wise to administer another right there. That was administered at the nursing home.
“After this second Treatment, I felt much better. I was feeling better all the time, then I would get a setback. Now, by a “setback” I do not mean every three weeks, but our reaction week. It might have missed on the third and hit on the sixth; it might hit on the twelfth, or miss me on the fifteenth, or something like that, but during the reaction week, I would feel badly. In other words I would not feel normal, like I did ordinarily, but after that reaction it seems to me that the severer the reaction was the better I felt afterwards and gradually my reactions disappeared and I felt better, more and more, oftener and oftener, and the first thing I knew I was feeling fine all the time.
“During this period my coughing decreased. My hemorrhaging stopped. I gained weight.
“I had a third Treatment about a year and a half later. I continued to improve.
“I do not recall exactly how many Koch Treatments I have had altogether, but I would say about eight or thereabouts. You see after my third Treatment I did not pay any attention whether I got one or not. I was feeling all right and if Dr. Koch gave me one, well, it was probably because it was his idea, not that I thought I needed it. These Treatments from Dr. Koch were given from about 1934 to March 1941 or 1942. I do not know exactly.
“After I left the Maybury Sanitarium and after I took the first Koch Treatment, I did not take any other treatments of any kind. I did not take any other therapy of any kind. Since the time of the first Koch Treatment, I have received no medical attention other than from Dr. Koch.
“I weigh 175 pounds now. I feel fine.
“My working hours vary. One day I work in the morning and the next day I work in the afternoon, but all in all I work about forty to forty-five hours a week.
“I do not cough now, I never raise blood. My appetite is fine. I do not tire easily. The general condition of my health is fine.”
Visitors to Stanley Sanchez’ gasoline station in 1950 report him still active and working hard every day.
ANALYSIS OF THE REBUTTAL OF THE STANLEY SANCHEZ CASE ATTEMPTED BY DR. BRUCE DOUGLAS
This case was classified by Dr. Douglas on page 7959 on direct examination as a far advanced case on admission in October, 1930. On page 7491 he testified for the Government on direct examination that Mr. Sanchez had received his benefit from the treatment received in the five years under sanitarium care plus the rest he received.
On cross-examination, however, he admitted that further treatment was necessary, removal of the lung or part of it or a revision operation of some kind. This was an admission that the patient was in most serious condition and that all of the previous sanitarium care including the thoracoplasty had failed to stop the progress of the disease and now the patient, in an exhausted condition, had to have an exceedingly dangerous operation as a last attempt to halt the infection.
The quotations from Wilson and Pinner given earlier show that little hope for benefit lay in that direction. He was surgically exhausted, the infection was not halted, mediastinal shift, and extensive adhesions made removal of the lung out of the question. The extensive fibrosis of the lung as revealed in the X-ray plate exhibits, removed any hope of collapsing such a lung so as to obliterate the cavities causing the hemorrhage and harboring the infection. But in addition the infection had reached the intestine and progressed in spite of careful surgery. Surely this man needed something more than the attack against the injuries done by the disease. He needed his defense mechanism restored, and his chemistry repaired so he could no longer harbor disease-producing germs. Since recovery followed the Koch Treatment rapidly and steadily until good health was reestablished, we are forced to conclude that the Koch Treatment offers the correct method of attack, and should be made available to all sufferers from tuberculosis that desire it.
Pulmonary Tuberculosis
THE CASE OF MARIE BLANCHARD HALL
Introductory Remarks
This is another case where cavity collapse was not accomplished during 3.5 years of hospitalization. Phrenectomy was performed. That is, the phrenic nerve was partly removed to paralyze the diaphragm. It is an operation that deprives the patient of the ability to normally cough out the germs and tissue debris that accumulate so rapidly in an advancing infection by the tubercle germ. The idea of the operation is to quiet the lung, but its value is now being doubted and it is also recognized as harmful in many instances.
At the age of twenty-four, in August 1931, Mrs. Marie Blanchard Hall caught a severe “cold.” Much coughing, fever, weakness, and raising of considerable sputum brought her to the Herman Kiefer Hospital (the City of Detroit Tuberculosis Hospital) where X-rays and sputum examination showed an advanced stage of tuberculosis. She entered this institution for their care and was also cared for at the Maybury Sanitarium, another municipal institution. The sputum stayed positive and the disease advanced.
To demonstrate the progress of the disease while at the Detroit tuberculosis hospita1s, four X-ray films were presented. The first two showed the condition when she entered the Herman Kiefer Hospital in August 1931 and in April 1932. After resting there a while she was transferred to the Northville Tuberculosis Sanitarium, another municipal institution. These films show the major tubercular deposits in the apex of the right lung. The next Film, No. 3, showed the state of this deposit in January 1934. It is evident that a large cavity has formed at this place. The lung tissue rotted out, to speak plainly. The thick ring represents the wall of the cavity.
Film No, 4 (Plate 5) shows the condition of this same region on March 8th, 1934, just three weeks before she left the Maybury Municipal Tuberculosis Institution. It is evident from the changes in this film that the disease was advancing. Thus the wall of the cavity has thickened and formed a nodular outgrowth that extended into the surrounding lung tissue. Moreover, the products of lung destruction have been piling up in the cavity leaving less emptiness. The films show these changes plainly. This nodular increase in the walls of a cavity is well recognized as a sign of uncontrolled progress of the disease. A smooth wall means, conversely, that the situation is improving.
PLATE 5. This X-ray was taken on March 8, 1934 in the Case of Marie Blanchard Hall, indicating that the tuberculosis was advancing.
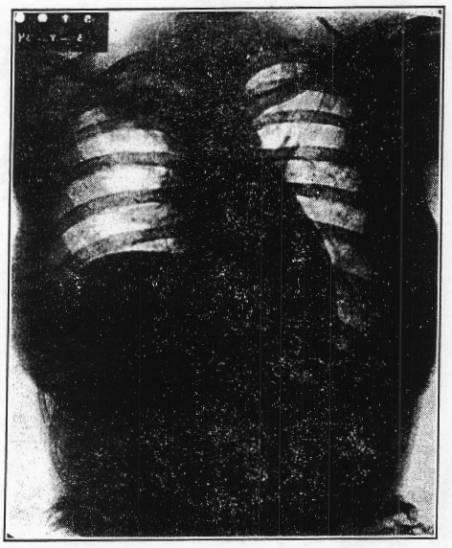
No film is accessible showing the condition when she left the institution, March 29th, 1934. For several weeks at this time the physicians there were trying to explain to her, as her Testimony shows, that she must have her ribs removed if she wanted to live; “thoracoplasty or death,” she reported to us, was their argument. She was running a fever that hovered about 104 degrees and “was a very sick girl” all this time, as she expressed it.
What the radiographs would have revealed at that time, had they been made, can only be conjectured from certain facts in addition to the condition revealed in Film No. 5 taken September 24th, 1934, six months after she left the institution and six months after she received her dose of Koch’s Glyoxylide, April 2nd, 1934. This film must be interpreted in the light of the important fact that she was in good health, physically strong, in good nutrition, no cough, negative sputum, strong, steady pulse, easy breathing, and normally not fatigable. The cavity is clean with smooth walls and surrounded by healthy lung tissue. It, therefore, is healing and though not yet replaced by normal lung tissue and healthy fibrosis, it is on the way with a good start. The cause is removed and not further injuring her. Thus healing can progress. That this did progress to completion is demonstrated in Film No. 6 taken a few years later and showing that the recovery is permanent. (Plate 6)
We must conclude that though the cavity is larger in Film No. 5 than in Film No. 4, it represents a stage of transition from a worse condition at the time she left the sanitarium and when thoracoplasty was considered urgent, and she was carrying a fever of 104 degrees, with rapid thready pulse, rapid labored breathing, yet cyanotic though flushed from fever, and presenting the picture of an acute tubercular pneumonia of a rapidly fatal military tuberculosis (galloping consumption). This cavity in Film No. 5 may reasonably be considered to represent an area of marked lung destruction that had not healed as yet, but was already free of infectious activity.
PLATE 6. This X-ray was taken on September 12, 1942 in the Case of Marie Blanchard Hall, eight years after taking the Koch Treatment. It indicates that complete recovery from tuberculosis is still maintained.
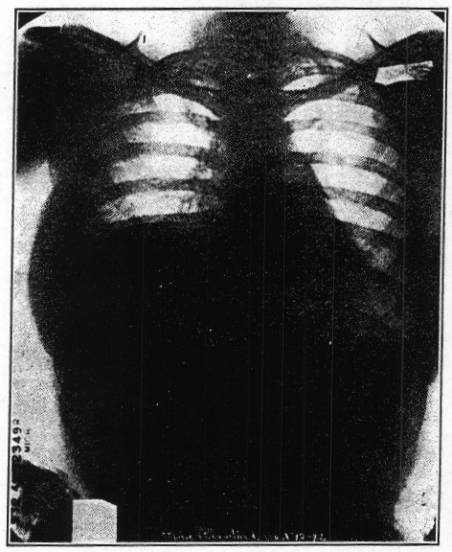
These characteristics demonstrated in the several films show that the cure of tuberculosis following Glyoxylide takes place before the cavity has healed. The disease cause is disposed of first and the cavitary defects are cleaned out and healed afterward, not by collapse, but by replacement with normal tissues. This is the ideal mechanism and the natural way that recovery can take place after the germs causing the disease are killed. Tests showed that long before Film No. 5 was taken the sputum was free of tubercle bacilli.
After the germs are destroyed, the fibrotic cavity wall can be absorbed for, since it is produced to imprison the germs and limit their activity, it is no longer needed. It can, therefore, be absorbed and replaced by lung tissue as is seen in Film No. 6.
The details of this case are presented in the patient’s own Testimony and extracts from the hospital records.
TESTIMONY OF MARIE BLANCHARD HALL DIRECT EXAMINATION
(Note: The following is paraphrased from the Testimony given by Mrs. Marie Blanchard Hall at the Koch Trial and which may be found on pages 6000-6010 of the Official Court Record. The words below are those of Mrs. Hall.)
“I was ill in August, 1931. I had a severe cold which I thought was a cold, and it was tuberculosis.
“I was sent by my doctor to have an X-ray taken and the report came that I had several spots on my lungs. After they took the X-ray, I entered Herman Kiefer Hospital. The doctor who sent me there was the one who took the X-ray. (Plate 7)
PLATE 7. This is a hospital record indicating the “far advanced” tuberculosis when Marie Blanchard Hall first entered Herman Kiefer Hospital in Detroit.
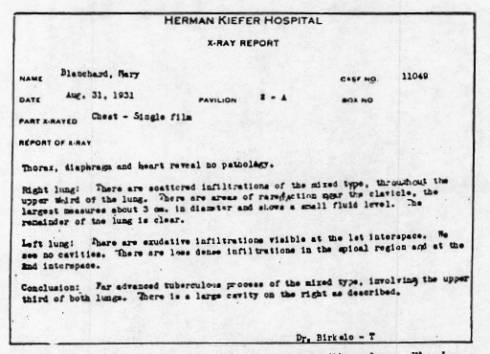
“I had bed rest after I entered there for about a month and a half and they suggested a phrenectomy, which I had. The phrenectomy was a pulling of the nerve and they cut it so as to make it permanent. They did not give me an anesthetic. They do not with the phrenectomy. It hurt very much. I will never forget. To my knowledge, I did not observe results from that operation.
“I remained at Herman Kiefer until May 12th, 1932. I did not feel any better after I left there than when I went in. I was coughing, and raising sputum. I was very weak. I went to Maybury Sanitarium at Northville, Michigan. I did not receive treatment there. I only had bed rest. My condition did not improve very much with bed rest.
” I remained at Maybury Sanitarium from May 12th, 1932 to March 31st, 1934. During this time I had nothing but bed rest as treatment. There was no change in my condition. I was still coughing and raising sputum. I had high temperatures off and on. I felt very weak.
“When I left in March of 1934, I asked Dr. Willis for permission to go home, which he did not want me to do. At that time I was raising a temperature up to 104 degrees. He refused but I said I could sign my release if I want to and he said, ‘all right, you are taking chances.’
“I did sign my release. I left right there. I came home and went to see Dr. Koch. That was March 31st, 1934. I received the Treatment on April 2nd.
“I noticed results from that Treatment after twenty-four hours. I woke up during the night with a sore chest and found it hard to breathe and almost thought I was dying. It was only a reaction, which I did not expect that was taking place and it lasted about one day, but I was very sick. I was not able to get out of bed, but after it lasted twenty-four hours, I was all right and I never had any severe reaction after that. I stayed at the nursing home six weeks after that first Treatment.
“I do not recall how long it was before I had a second reaction because it was so slight that I would not remember. It is twelve years ago, so I would not remember very much about it. I do remember the first one because it was so severe.
“After the reaction had passed I felt grand. I felt like I could live again.
“After I left the nursing home I went to live with friends in Berkley, Michigan, to get fresh air and rest, but I waited on myself and did all my work. I remained at Berkley from June to October, the same year, and after that I left there and came to live with my sister from October until the next May, which was 1935 and in May I went to work and I have been working ever since. I worked in a factory all the time and before I was married I did housework. I worked during this last war; did war work and bench work and different jobs on the bench. That was right in the factory. The conditions in the factory were not so healthy. It was dusty, because we were piling steel tubing.
“I had about three of Dr. Koch’s Treatments. I have not had any other treatments medically since I first took Dr. Koch’s Treatment.
“I do not have any cough at all and I do not raise sputum. I feel fine. I have felt well for twelve years. My appetite is very good. I weigh 134.”
(Note: Mrs. Hall has been observed in good health as late as June 1950. She is working daily and also maintains her home.)
AN ANALYSIS OF THE REBUTTAL OF THE MARIE BLANCHARD HALL CASE ATTEMPTED BY DR. BRUCE DOUGLAS
On Direct Examination, page 7469, Dr. Douglas testified for the Government that when this patient left the Maybury Sanitarium in 1934, the chances of recovery were favorable and on page 7873 he testified that the Koch Treatment had no effect because the recovery, which took place in that case is that which would be fully expected from a case that had this rest in addition to the sanitarium period.
You will observe in the case history that this patient, both according to her own Testimony and that of Dr. Koch, was in a condition which is found after a serious breakdown and the disease is on the gallop, such as in a widespread tubercular pneumonia or acute military tuberculosis. She could not even be moved safely for X-ray examinations. Patients in this condition are dying from tuberculosis.
On page 8058 and 8066 Dr. Douglas testified the patient needed further treatment and thoracoplasty would be necessary. In other words, the favorable prognosis given on direct examination is reversed on cross-examination when the full situation was brought to Dr. Douglas’ attention. The Testimony shows then that Marie Hall was drastically in need of help when she was given the Koch Treatment. Her recovery shows the help was real and efficient.
Acute Military Tuberculosis
WITH TUBERCULAR MENINGITIS AND SPONTANEOUS RUPTURE OF LUNG
Introductory Remarks
Another form of tuberculosis, the most rapidly fatal type, may develop on an infection previously established where the resistance is not good and a further breakdown permits widespread infection to develop through the blood stream; so that millions of new foci are set up all over the body, including the lung structure generally, the brain, bones, the spleen and kidneys. This event is made possible by the rupture of a tubercle into a blood vessel so that the infected caseous contents, with its billions of germs, are distributed to all the rest of the body.
THE CASE OF NORA ALDRICH RINEHART
A case of this type is reported here. She was a girl of 14 years when treated back in July 1922. She had been in the Detroit Tuberculosis Sanitarium about six months previously. (Plate 8) She tended to run high temperatures from 102 degrees to 104 degrees from the entrance into the hospital up to the time she left and thereafter. The radiographic findings at the time of entrance into the hospital on January 30, 1922, are available for study. They show the lesions to be of the rapidly disseminating type.
PLATE 8. This document indicates the official sanitarium diagnosis of “advanced parenchymal tuberculosis” in the Nora Aldrich Rinehart Case, six months before taking the Koch Treatment.
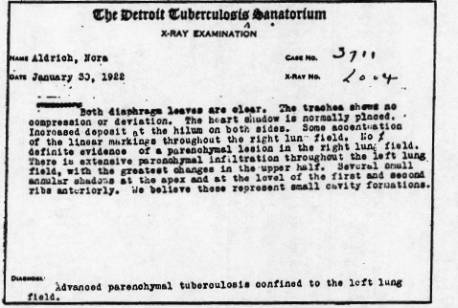
At the time of Dr. Koch’s first visit, she was emaciated, bedfast, in a stupor, comatose, had been vomiting projectively for three weeks, was cyanotic, with rapid weak respirations, very rapid, thready practically uncountable pulse, and with head drawn back stiffly, in a continuous spasm. The physical examination showed the heart to be drawn over into the right side of the chest; the left chest was empty so far as recognizable lung tissue was concerned. It contained fluid that could be heard to splash when her body was shaken. No breath sounds or signs of a lung could be found in the left chest. The lung had spontaneously ruptured. The right lung showed consolidations and cavities, an especially large one near the right axilla. The abdomen revealed a large tumor in the region of the spleen and left kidney. Whether it was a large tubercular spleen or large tubercular kidney could not be differentiated at that time. It could have been either or even both. At any rate she was dying. To better understand the seriousness of this condition a few authoritative statements are given, for comparison with the facts in this case.
(a) She was a young girl at the age when the disease develops most rapidly.
“The mortality rate is generally low between the ages of five and adolescence when there is an abrupt rise, reaching its peak in females in the early twenties and somewhat later in the males.” Cecil, “Textbook on Medicine,” page 315.
(b) She reacted with prolonged fever. All the time she was in and out of the hospital and when she was seen by Dr. Koch the fever was 105degrees.
“Clinical symptoms measure in an approximate degree the patient’s reaction to the infection. Thus, a young girl who reacts with prolonged fever usually ‘does badly.’
“Young tuberculosis girls have notoriously unstable lesions and the mortality is relatively high; there is a similar trend, somewhat less striking, among young boys.” Cecil, page 341.
(c) She had a spontaneous rupture of the lung, which is so quickly fatal.
“Most of these patients die soon after accident (perforation). Of Sauerbruch’s fifty-seven cases, forty-three died within a week. In our series of twenty-one patients with permanent perforation, only two with open drainage are living, one and four years after the accident, and in each the fistula is still open.” Packard, Hayes, Blanchet, “Pneumothorax,” page 155.
(d) She had the generalized military form with the fatal meningitis.
“In the acute generalized military form, the lungs are quickly and uniformly seeded with small tubercles, which as a rule do not ulcerate because death intervenes.” Cecil, page 324.
“Death occurs usually within six to eight weeks, occasionally with meningial involvement.” Cecil, page 355.
The Glyoxylide Treatment was given in July 1922. The recovery was rather rapid. The vomiting ceased, the spasticity of the neck and opisthognathous disappeared. She was able to take nutrition again and she gradually recovered. The heart stayed on the right side for over a year longer, and the pulse was very rapid for about two years. But gradually the heart began to come back during the second and third years after Treatment and the pulse slowed down. This slow return of the heart to the left side shows that much more repair had to take place than the difficult job of healing a ruptured lung. The elasticity of the lung was greatly reduced by generalized tubercular invasion and fibrosis, and by the vascularization that temporarily replaces the lesions preceding the formation of functioning lung tissue. This necessary process kept the lung solid for a while and together with fluid kept the heart from going back in place. Steadily, however, she normalized and some years later was married. She has two healthy twin children who are exceedingly resistant to infections and especially to the epidemic infections that affect the other school children. Thus a hereditary resistance has been handed down. She has remained a picture of health all these years, very active and well. The radiographs show her lungs to be normal and also show signs of the extensive healing that was required to overcome the terrible destruction that once laid them waste. The large tubercular kidney (or spleen) absorbed completely and physical examination reveals no trace whatever.
AN ANALYSIS OF THE REBUTTAL OF THE NORA ALDRICH RINEHART CASE ATTEMPTED BY DR. BRUCE DOUGLAS
Dr. Douglas gave the “opinion” that this case did not present a true tubercular meningitis but rather an irritation of the meninges by the poisons present, a condition which he called meningismus. He also gave the “opinion” that the large mass described by Dr. Koch as possible tuberculosis of the kidney was rather an accumulation of pus in that region.
Regardless of these interpretations, the fatal state of the girl, presenting enormous lung destruction, spontaneous rupture, extreme toxicity, could not be denied and her recovery was equally phenomenal.
However, an advanced case of tuberculosis of this type presents an overwhelming infection by the tubercular bacillus, and any injury to different organs could not escape influence by this germ. Moreover, the most likely hard, irregular enlargement occurring in the region of the left kidney, in such a case, is either tuberculosis of the kidney or tuberculosis of the spleen. This, Dr. Douglas carefully avoided mentioning. This large tumor could have been tuberculosis of the spleen and no alternative diagnosis given by an expert could properly escape mentioning this fact. To rule out ordinary pus infection, one must recall that such infections are not only highly fatal when so extensive, but they cause severe pain requiring large doses of opiates. An examination of the infected area by palpitation must cause excruciating pain. These were not present in this case so Dr. Douglas’ “opinion” was not in accord with the facts with which he was acquainted. Whether or not meningismus or meningitis was present Douglas had no way of determining except that meningismus does not cause the projective vomiting, which was present in this case. So, it would have been more proper, in view of the facts, to leave the designation as tubercular meningitis, which is so often a complication of a terminal case such as this.
This was the most serious case of tuberculosis ever described that recovered, as far as we can determine. This recovery followed one administration of the Koch Treatment.
Tuberculosis of the Spine
Introductory Statement
Tuberculosis of the spine is one of the most hopeless and pitiful forms of the infection. Occurring in children so often, the little things start out on life with intense suffering and privation. Nothing is so pleasing to a human heart as to see a cure of this terrible disease by a truly scientific approach, so that the orthodox course of treatment, which is usually unsuccessful and very miserable, can be avoided.
The usual treatment depends upon absolute rest and immobilization of the affected bones. To secure this the patient must be always lying down on his face or flat on his back. He is strapped in a shell or other contraption that fixes the spine absolutely and removes the weight and pressure from above the lesion. If he is to be turned, he is turned carefully in one piece, as it were, so that no motion will develop between the bones about the lesion. Otherwise, he is not allowed to turn or move from his position. He is so held two or three years as a rule.
Surgery may be performed, either the Albee splint operation or some other, the object of which is to transplant bone into spinous processes to fix the bones immovably. Even though this is performed, an additional year or more in bed is required with the patient flat on his back. The correction of the hump or deformity is not expected and does not take place either, except perhaps to a minor degree. Healing of the lesion with immobilization of the affected parts is all that is expected, but it only too often does not occur and the patient goes on through his torture to a miserable death. There is no satisfactory ambulatory method of treating tuberculosis of the spine known up to this demonstration of the value of the Koch Therapy.
It might be enlightening to quote some of the leading American authorities:
“Immobilization of the spine accomplished by the rest in bed, support on a firm frame, plaster shell, or brace until healing by bony consolidation of the diseased area is complete. Prolonged recumbency is necessary.” Christopher, page 437-8, Saunders & Company, 1945.
“The angulation, hump, or kyphosis deformity are not corrected by the orthodox method but are encouraged to persist to keep the remaining parts of the crumpled bones together, so as to favor union.”
Philip Lewin, Prof. of Bone and Joint Surgery, Northwestern University, Chicago, in his textbook, “Backache and Sciatic Neuritis,” Lea Febiger and Company, 1934, 1944. Page 288-289, states:
“If a khyphos (hump) has developed, due to the collapse of vertebral bodies, it is not wise to try to correct the deformity by quickly forcing the collapsed vertebral apart. Prevention of the collapse is warranted and should be attempted but an empty space should not be produced ‘in the anterior column healing by solid bony fusion in the diseased area requires a long period.”
“In children with tuberculosis of the lumbar spine, when the process apparently has started in the disc and has invaded contiguous areas of the vertebrae, solid bony fusion will often result in two or three years, without operative influence.”
“Spontaneous fusion requires, on average, over six years. “Patients who have definite evidence of metastatic involvement have a mortality of almost 70% and no surgical treatment other than emergency measures to relieve pain or abscess should be attempted.”
(The next case, the Aldrich boy, was a metastatic case as the evidence shows.)
“The best results are obtained when patients are carefully selected for operation, when spine fusion is employed during the period of healing of the disease and when such treatment is supplemented by conservative treatment for a prolonged period.”
“No surgical treatment can be considered a substitute for conservative treatment.”
Swett, Bennett, and Street, “Bone and Joint Surgery,” Vol. 22, page 678, 9940, conclude:
“After an indefinite length of time the lesion may heal, but in a large number of cases healing fails to occur.” “Even when healing does occur the time during which the process often remains unhealed is long. About one-third of the patients die within a few years. There is no advantage in the operative treatment over the non-operative.”
THE FOLLOWING DATA IS PARAPHRASED FROM DR. KOCH’S TESTIMONY GIVEN ON THE JAMES ALDRICH CASE
The present patient was a child of three, when he was seen by Dr. Koch in August 1925. He had a definite hump in the lumbar spine. He wore a tight brace that made it possible to walk. He had been to the leading orthopedist, Dr. Laferte, Sr., before being brought in. This specialist fitted his brace and advised placing him on a frame for at least a year and possibly an Albee splint operation to immobilize the vertebrae that were attacked. There was much muscle spasticity about the diseased area. No radiographs were made at the time, since those taken by the orthopedist were available, however, these are not available now twenty-one years afterward and one must rely on what the healed spine shows to demonstrate the pathology that existed formerly.
“This radiograph taken for the Federal Trade Commission Hearings, absorbed in part and fused together to make the spine one vertebrae too short, however, there is no hump and the bodies of the vertebrae are in perfect alignment in all directions. Hence there is no distortion, in one of the upper thoracic vertebral bodies an area of density exists the size of a large pen showing where another lesion had started and was healed before it could do injury. The very dense bone making up this repaired area shows the nature of the process of healing. (It also shows this to be a metastatic case, the type with 70% mortality rate according to Dr. Phillip Lewin.)
“The history of the case is that of pain starting at night when he relaxes in his sleep. Later he could not move without pain and if he fell down he could not get up. The condition was quite advanced when he was brought in and a different brace was fitted, which was worn for about six months. It was rather loose, but kept him from making gross changes in posture when sleeping. It did not relieve the diseased area of the weight of the body nor did it keep the diseased bones from moving, as is required by all accepted rules for care of these patients. It did not relieve the pain entirely either. Thus the brace, which was worn only six months, protected him while at play from serious fracture, and also limited his movements at night during sleep, and reduced the muscle spasm about the lesion.
“The Glyoxylide was injected immediately. This was done in August 1925. Recovery was quite rapid. In six months he refused to wear the brace and could walk and play without it. The hump had disappeared and so had the spasm of the muscles of the region. The spine appeared definitely shorter, however, he grew up like other children, played their games, and has maintained good health ever since.”
TESTIMONY OF JAMES ALDRICH BEFORE FEDERAL TRADE COMMISSION HEARING
“The first thing I remember in my life is when I was three years old. I went to my uncle’s cottage that summer. It was shortly after that time I started having pains in my back. I remember my father taking me to the chiropractor and I remember my father said I had a dislocated spine. I was taken to several other doctors. I remember X-rays being taken. I remember Dr. Koch giving me a shot. I remember wearing a brace. It inhibited me, when I fell down I could not get up. I wore it all day for four or five months, then my mother finally consented to taking it off at night and not long after that I stopped wearing it altogether. (Tells incident of getting up and walking without the brace. About a week after that, he wore it no longer. No trouble with back after that.)
“I believe I was still wearing the brace when I started in Kindergarten. I was wearing it when Kindergarten opened and perhaps in September or October. I do not think any longer than that. As nearly as I can recall, I discarded it finally about the first part of November 1925. I think when I started to Kindergarten was when I was just wearing it days. My mother had taken it off that summer. I was particularly uncomfortable in hot weather and it was that summer she started removing it at night.”
Here again is a demonstration that recovery is secured by getting rid of the cause of the disease, not by killing germs by a powerful germicide, but by a harmless process of restoration of the natural immunity of the body. Thus recovery took place and the dead bone debris was cleaned out as the result of getting rid of the infection. This gave Nature a chance to repair the damage in a masterly way. She absorbed whatever bone interfered with proper alignment so that no hump remained and the whole spine carried the body weight perpendicularly. This is an entirely different result than occurs after orthodox methods, or spontaneously so to speak, which leave the deformity, or even accentuate it. Even at that the patient is lucky to get out of the trouble in this deformed condition.
Since the X-rays in the hands of the Federal Trade Commission are not available to us at this time, we have others that are not so well made, and are not large enough to show the metastatic lesion in the thoracic vertebra, which is shown in the Federal Trade Commission films. Yet they show the bone absorption, the evening off, and the perfect union, where the lesion formerly was. They also show that the hump is no longer present. An incident occurred in giving the Testimony in this case; Dr. Koch did not have the history of this case with him, since this was taken about twenty years previously, and was misplaced. He therefore had to give the history from memory, and misstated the year in which Jimmy was treated as being in 1923, instead of 1925. Dr. Koch on returning home from Washington where the Testimony was given, found evidence that he made this error and asked the privilege of correcting it. However the Federal Trade Commission attorney refused with the words, “Not in your life will you correct it, except over my dead body.” Of course, the matter was too trivial for such an event, yet it shows how a truth-finding commission, as the Federal Trade Commission is supposed to be, hates the truth when certain interests are not favored by truth. It might be added that the Sur-rebuttal requested by Dr. Koch, to show up the errors and falsehoods of the Government’s rebuttal, “opinion”expert witness, was denied him by the presiding judge. In matters of soapboxes and neckties such refusal to get the truth the whole truth and nothing but the truth would not be so serious, but in matters of health, suffering, and life and death, a very serious situation exists. Here the whole truth is important regardless of the consequences.
AUTHOR’S ANSWER TO THE REBUTTAL OF THE JIMMY ALDRICH CASE ATTEMPTED BY DR. BRUCE DOUGLAS
The Rebuttal in this case was that the brace, which Dr. Koch employed for a few months, actually brought about the recovery. It must be recalled that this brace was loose, that it did not keep the weight of the body off of the diseased bone and it did not prevent motion at that area. Please refer to the quotations from the authorities a few pages back. It is emphasized there that absolute immobility must be maintained, that if the patient is to be turned over it must be done as one piece and that the shell or cast which holds him absolutely rigid is made for that purpose. Then, it requires years of such immobilization to secure an occasional fixation of the parts, with the kyphosis (hunchback) deformity still present, or even emphasized.
Contrast with this the rapid healing while the child was running around and the absence of a kyphosis deformity; the spine actually straightened out with recovery. Thus, the recovery under the Koch Treatment was different in every respect from the best results obtained by immobilization.
Dr. Douglas’ Rebuttal, therefore, does not conform with the facts or with authoritative opinion.
LET US GO on with the mechanism of producing cancer as Koch views it, and explain how he arrived at some of the important facts that feature his research. This exposition may require a little repetition for clarity. The delicate fibrils that make up the oxidative functioning mechanisms may be injured by mechanical means* and, of course, by the exhaustion of fatigue. Injury reduces or destroys the power to burn sugar energy and then the cell must resort to a more primitive and far less efficient means of securing energy, namely, glycolysis, which is the splitting of glucose to lactic acid. This is the process used by cancer cells that have lost their functioning mechanism and by embryonic cells that have not yet developed one.
For many years, the biochemists recorded the figures showing lessened oxidation and increased glycolysis from injury when tissues are cut in thin slices for studying in a Warburg Chamber. But the fact that mechanical injury reduced the oxidative powers was not recognized except by a few scientists, such as Roger Williams.
(*Anti-oxidants arising in the intestinal tract, automobile exhausts, chemicals present in coal tars, incompletely oxidized germ products, and synthetic carcinogens.)
The glycolysis process does not provide the substances that are able to induce the oxidation of poisons that produce cancer, mal-developments, or other disease. Now as Dr. Koch pointed out, mechanical injury or chemical fatigue injury by stopping the oxidation process robs the cell, be it tissue or germ cell, of the power to burn an antioxidant to harmlessness and this antioxidant can then remain in the cell unchallenged and unchecked in conducting any disturbance it is able to produce.
Dr. Koch showed that the double bonds between carbon atoms and between nitrogen atoms, not only confer the antioxidant properties, but also the particular fluorescence that produces the specific pathogenic action of the substance.
He also saw in these double bonds the means of destroying the specific pathogenic structure and action. Fluorescent substances have the ability to absorb the energy from exothermic reactions going on in the field and emitting this energy at a lower grade from that received. They can thus stop the progress of a chain reaction by blocking the energy required for the next step. Thus, they are able to stop a special cell function and produce what is known as an anargy, or suppress normal development, or cause an atrophy.
But should this absorbed energy be emitted at a level where it can be accepted by some functional mechanism, it passes into the chemical processes of this mechanism and forces that function in a way that is not under physiological control, and so some forms of allergy are brought into being.
If the contractile mechanisms of a system of tissue cells accept the energy, spasms as of asthma arise. If the secreting fibrillae of the cells of mucous membrane accept this energy, uncontrolled secretion as of hay fever results; if the conducting fibrils of a system of neurons of the nervous system accept the energy, fixed ideas of insanity, the compulsions of a neurosis, or the spasms of multiple sclerosis, epilepsy, etc., come about.
It will then be evident that the fundamental cure of all these disease expressions is the induced oxidation destruction of the causative toxin, but this had to be done by supplying the catalyst that will restore with proper vigor the normal oxidations in the affected cells, as we have already ascertained.
And so Dr. Koch used this double bond fluorescent property of the toxin, which he announced years ago, for the oxidative destruction of its injurious powers. Is it not interesting that today, just in the last three years, the fluorescent factor in cancer is being photographed and reported in the scientific journals as a great discovery? Confirmation of the correctness of Dr. Koch’s work is springing up on all sides.
THE CASE OF RITA LONG
The highly fatal retinoblastoma, (glioma of the eye) that attacks children from two to four years of age, has also been cured following the Glyoxylide Treatment. The case here presented is especially interesting in that both eyes were affected. This disease is one of the outstanding examples of a specific tumor process with a characteristic clinical history, as well as characteristic structure and thus, is readily diagnosticated. (Ewing, p. 470, Duke Elder, Vol. 11, 1938, p. 1337-1377, Vol. III, 1940, p. 2168-2170, May, p. 208, 233, 299, 1941).
The Case of Rita Long — This child gave the first symptoms of loss of vision as observed by the parents in March 1934, when she was fourteen months old. It was evident that the left eye had become blind. An expert, in diseases of the eye, examined her and the diagnosis “glioma of the retina” was made. The eye was removed and the diseased tissue was observed to involve the optic nerve region. The right eye at this time was found to be normal, but several months later the same trouble started in the right eye and progressed in exactly the same fashion as in the eye that was found to be cancerous.
The same specialist examined the right eye and found exactly the same condition that made it necessary to remove the left eye. However, the right eye was not removed nor was it subjected to X-ray treatments, as the specialist suggested. Instead, another eye specialist was consulted and he recommended that the child be given the Glyoxylide Treatment. She was brought to Detroit to Dr. Koch’s Clinic.
In as much as twenty-three percent of such cases develop glioma in both eyes, and the disease is so highly fatal, the results that followed the Koch Treatment are most gratifying.
The Glyoxylide was given on November 25th, 1935, and a second dose was given August 18th, 1936, after considerable improvement was evident. The eye stopped being irritated and the paralyzed, dilated pupil soon normalized, the vision returned, and recovery was complete within a year. During the recovery process, reactions occurred every three weeks. They were characterized by general grippiness, and some irritation of the eyeball, and sometimes by fever. Each reaction became successively lighter and following each there was a more definite improvement. This went on until recovery was complete. This patient is a young lady now in good health and with a good healthy eye that has good vision.
The hospital record contains the data about the operation and microscopic findings. The results of Dr. J. O. Cheney’s examination of the second eye, and Dr. Hugh’s examination are also given.
Dr. Cheney who removed the left eye after making a diagnosis of glioma (blastoma retinae or retinoblastoma) described his diagnosis and operations as follows in this paraphrase:
He examined the child in the spring of 1934, and found the eye blind and painful due to increased tension, which is caused by this type of cancer and from his examination he made the diagnosis of glioma of the retina. He removed the eye and the pathologist, Dr. Harold Palmer, examined it. His report shows the external and internal appearance of the eye and the microscopic findings. On section, the posterior chamber was practically filled with a grayish friable tumor mass, which seemed to be attached to the region of the nerve head. The pathological diagnosis was glioma of the retina.
In November 1935, the child was again brought to him complaining of dimming vision and ophthalmoscopic examination showed, “what I believed to be a similar condition to the one which had existed in the left eye,” he explained. He advised X-ray treatments, but the parents refused this and brought her to Dr. Koch.
TESTIMONY OF MRS. BONNIE MANN
“Mrs. Long is my sister, and I have known Rita since she was born. I saw her very often. One time it happened that the light was thrown in her face just at the right angle to show a yellow light in her eye, and that eye was bulging and out of focus. I blurted out that she was blind. I could see the blindness. I saw her often at the hospital, and watched the other very closely because I was afraid it would come back. I saw the same thing in that eye, except it wasn’t as bad as the other eye, the first one. It wasn’t bulging as much. It was slighter than the first one. You had to look a little closer to see it. I took her to Dr. Cheney that day, and he told me to bring her back the next day, but I didn’t take her as they had already planned to take her to see Dr. Koch.”
THE TESTIMONY OF MRS. MILDRED LONG
“My daughter, Rita, was born in 1932. By the time she was a year old, I noticed some difficulty about her eyes. I noticed a reflection of light upon the eye, and a sort of a whiteness to the eye reflected the light. This was the left eye. We could see the change all along. We could tell that she had no vision in that eye, by covering the eye that seemed to be normal and then passing our hand over the eye that was affected. When she was two years old, I took her to an oculist here in Wichita, Dr. Cheney. She was taken to the hospital, and an enucleation of the eye was performed. She recovered from the operation. Sometime later, when she would wake up in the morning she couldn’t see plainly; it seemed as though there was ‘dust’ in her eye. She would rub her eye, and this ‘dust’ would seem to move. That is, it would come and go. It lasted several minutes. This was about a year and seven months after the operation. She was taken back to Dr. Cheney by my sister.
“We went to Detroit to see Dr. Koch, and stopped on our way to see Dr. Bonine in Niles, Michigan. Dr. Koch examined Rita, and we took her to a nursing home there, and she had the preparation that was recommended for the Treatment.
* Wichita Hospital *
PATHOLOGICALREPORT File No. 4120
Name Long, Rita C.
Room 111.
Case No. 1-2468
Age 23 mo.
Sex F.
Race W.
Surgeon Dr. Cheney
Examined by Harold W. Palmer.
Pre-Operative Diagnosis: Glioma of the eyes
Post-Operative Diagnosis: (not readable )
Gross Pathology: eyeball having a normal external appearance. On section, the posterior chamber is practically filled with a grayish friable tumor mass, which seams to be attached to the region of the nerve head.
Microscopic Pathology: Section of tumor shows rounded dark staining nuclei of cells practically devoid of cytoplasm set in a thin connective tissue stroma having no characteristic arrangement. Marked necrosis is present in some areas and round cell infiltration may be seen in some areas. Section of nerve head shows no tumor tissue.
Pathological Diagnosis: glioma of retina.
Signed,
Harold W. Palmer
PLATE 9. This is a Wichita Hospital pathological report in the Case of Rita Long, demonstrating that she had “glioma of retina” which was a cancer in the left eye. The eye was removed.

“She was given the Treatment, and remained in the nursing home three weeks. There were changes; nothing dramatic, no big change at the time, but she would seem to be responding to the Treatment in various little ways. She didn’t have the ‘dust’ in her eye while we were there.
“During the reactions she would have the same symptoms that she had before the Treatment was given; recurrence of this ‘dust,’ colds, just generally seemed to feel bad, and we thought at times that she had a little pain in her eye. Each time the reaction would subside, she would be definitely better.
“At the end of three years, we felt that she was all right. Of course, long before that, the eye apparently was all right, but there would still be these reactions and minor occurrences of some of the symptoms. We followed the diet very rigidly for three years. She started to school at five, and has gone to school right along. She is an A student. She has had glasses fitted to her, and she wore them for reading and close work, but the last time her eye was examined they thought she didn’t really need them, but I felt for close work, perhaps it would be better, so we had them fitted again. A year or more after the first Treatment, Dr. Koch gave her another injection, and she had another in Florida two years ago.”
TESTIMONY OF RITA LONG
“I am in the seventh grade and I got all A’s. I always tie for about top or second in my grade. I rarely study at home because I can get my lessons at school. I read library books at home. My eye never bothers me at all, and I read everything the teacher gives me. I have no trouble seeing motion pictures.”
TESTIMONY OF MR. ROMAINE G. LONG
“I am the father of Rita Long. Rita was born May 29th, 1932. At about the time she was one year old and even previous to that, I observed something unusual in Rita’s condition. It was quite gradual at first. Her left eye appeared weak and there would be intervals when water would discharge from her left eye and as time progressed that became more of a matter of course and there would be times when she would wake up in the morning that her eye would be entirely sealed shut with this maturation, and I would say it was at that stage after she was a year old.
“She would a lot of times, even though she was very small, rub her eye quite a little and we noticed, or imagined that we noticed, an enlargement of the left eyeball and she would complain of ‘dust’, and was quite irritable at times indicating that there would be something wrong with her eye. After this had progressed to such a degree we could see in the optic part of her eye instead of being dark it was white, such as a plastered wall. We would look in there and we became quite concerned about it. At different times I had made tests to satisfy by covering her right eye and moving my hand in front of her left eye to see if there was any reaction. At one time, I finally concluded that there wasn’t any vision there. Before this we had wondered quite a lot if there was anything wrong. But, after we found that the vision was entirely gone, that was when we became concerned and took her to an eye specialist in Wichita.
“The specialist that saw Rita at that time was Dr. Cheney. He was located in Wichita, Kansas.
“He examined the eye and said it was glioma and suggested an operation for removal of the eye the first of the following week. This was on Friday. At that time Rita was hospitalized, and received surgery. I do not remember the exact date of the surgery, but it was the forepart of May, before she was two years old.
“The wife and I both were in the operating room and saw the removal of the eye.
“Her condition, generally speaking, immediately following seemed quite normal. However, in the meantime we were concerned, naturally, and had done some investigating and inquiring and learned quite a bit of the character of the disease that she had and to satisfy ourselves, intermittently at regular intervals of about every sixty days, took her back to this same doctor for an examination.
“After time progressed, and I believe it was in the neighborhood of a year and a half, we took her again to this same doctor for an examination after she had complained about ‘dust’ again and her eye acted the same as the left eye, by watering; and later, as it progressed, there was some maturation. We took her to this same doctor and he found a growth, as he explained it, the recurrence of the same growth as far as I know.
“After that examination, he suggested that we submit to a series of X-ray treatments; that, in our investigation from what results we could find on records, did not satisfy us. We had in the meantime heard of Dr. Koch of Detroit. The wife and the daughter and myself and my mother and father got in the automobile and we came to Detroit to see Dr. Koch. It was a short time before Thanksgiving Day in 1935.
“On the occasion of our visit to Detroit, Rita received a Treatment from Dr. Koch. It was a hypodermic injection in her hip. I would say the first results came after two weeks. After the Treatment was given, we stayed three weeks. At the end of this three week period, we observed, that is, the wife and I and also Rita that she complained of being chilly or cold and we noticed on her body little red spots, both on her stomach and on her back. We took her then to see Dr. Koch and he examined her again and was satisfied by his expression that she was reacting, so we went back home.
“After we arrived home, the wife continued with the diet for the daughter and at these various intervals she would become quite sick.
“At different intervals, she would become quite sick and even her right eye would maturate as it had previous to coming to Detroit. Each time it seemed, however, that these periodic sicknesses would become worse until eight or nine months after she had taken her first injection. Each and every time, however, between those times it would become quite noticeable that her eye was much clearer and there was not any watering or maturation other than these times. They were so severe at two or three times that I even called Dr. Koch on the phone to talk to him about it. I thought it might be that she was maybe becoming worse or as bad as she was before we went to Detroit, but he would check the time the injection was given, and in a very consoling way would say, ‘That is very fine, that is just what we want. We expected that.’
“All of this time, he insisted that we not have any examination by using any other medicine or any other light, severe light, because of the delicacy of the eye. Then the wife and daughter came back to Detroit. I am not sure of the date. It is my understanding that she did get her second Treatment at that time.
“After the first Koch Treatment, it seems to me, it was in the neighborhood of eight or nine months before she did not have these terrible reactions.
“She has never had any other treatment but the Koch Treatment, since she first received the Koch Treatment.
“Rita will be fourteen the 29th of this month, May. She attends school regularly and she reads normally.
“I notice nothing out of the ordinary in observing her eye now. It is perfectly healthy, as far as I can see. She has not complained at all, not in the least. It is about seven or eight years since Rita last complained about her eye.”
(Communication from the Long’s as late as 1953 indicates no recurrence. Rita’s eye is in excellent health. She was married this summer.)
No fact Testimony could be secured by the Government to rebut this case. They canvassed numerous experts and placed the facts of the case before them, requesting them to try to rebut the facts or give “opinion” Testimony to the contrary; but they were turned down. In the second trial, no rebuttal whatever, not even “opinion” Testimony, was offered.
PLATE 10. This is a confirming letter, from a Detroit physician, showing that Rita Long had a tumor in her right eye when he examined her on November 31, 1935. This eye was saved by the Koch Treatment and is normal to this day, more than twenty years later.
RAY W. HUGHES M.D.
April 18, 1935
“To whom it may concern:
“Rita Long, a 3-½ year old female of Wichita Kansas, was referred to me by Dr. G. Warnshuis, on November 31, 1935 with a diagnosis of glioma in the right eye.
“Ophthalmoscopic examination revealed a flattened white mass penetrated by blood vessels, six or seven times disc diameter in the upper right nasal quadrant.
“The left eye had been removed for glioma nineteen months previous to this examination.
“I have never seen the patient since.
“Yours very truly,
“Ray W. Hughes M. D.”
The “opinion” Testimony offered in the first criminal trial was produced by the expert at the University of Michigan. His Testimony is exceedingly valuable — in that it shows there is no method known to him whereby this disease can be controlled. He testified as follows: (page 1149 transcript)
“Another type of cancer which we see too much of and have no control over is that type which no doubt most of you read about in the newspapers a few years ago. An instance in Chicago where a child was affected with a tumor and the other eye was also affected by this tumor, and the great question arose as to whether both eyes should be removed, whether the parents would rather have a child with… (interruption)
“I am going to give an example in just a few minutes, sir. As to whether both eyes should be removed in an attempt to have a blind but living child, or whether one eye should be removed and the other eye given X-rays, or whether no operation should be done at all.
“We had just about two months ago in our clinic a little boy who was sent down by a doctor from the northern part of the lower peninsula because he had a tumor in his eye.
“This tumor we call retinal blastoma, sometimes called glioma. This type of tumor affects children, usually within the first three years; sometimes they are born with it; and this is probably one of the most malignant tumors in childhood.
“Therefore, we took the eye out of this little boy, as the only possible hope that we had of saving his life. Examination of that eyeball showed no evidence that it perforated the outside of the ball.
“The examination by the pathologist showed that it had not established beyond the optic nerve where it was severed. So, we had the best assurance by the best means we knew that the tumor had been completely eradicated. However, no one knows whether that tumor had spread to the other portions of the body.
“He came back last week or the day before yesterday, and we found he had a recurrence in that orbit and the mass which had filled the orbit there was as large as the former eyeball. When that occurs, the chance of saving this child’s life is practically nil. There are few things one can attempt. You can only hope that it had not spread any further than the optical tissues.
“We remove the contents of the orbit — it leaves there a hole in the child’s face almost large enough to put a fist in and no plastic function will restore the child’s function. There is no treatment, X-ray or anything that we know of in scientific work that can fight this.”
Fact Testimony could not be produced to rebut the fact that Rita Long completely recovered, and so it still is, twenty years after she received the Treatment. Furthermore, the affected eye, which was not removed, has returned to normal and the eye functions perfectly.
The process of recovery with its three-week cycles of reactions clearly shows here too that the recovery was a feature of the Koch Treatment.
EXTENSIVE CANCER OF THE STOMACH RECURRENT AFTER OPERATION
THE CASE OF MR. WESLEY ROEBUCK
Introductory Remarks
It is well known that when cancer of the stomach is first recognized after it has caused definite clinical symptoms, it is too far advanced to be cured by operation. This is true always of the types that metastasize early and infiltrate widely and vigorously. Two such cases are here given:
One, a farmer, age sixty-nine, was operated June 28th, 1926, in the attempt to overcome obstruction of the lower end of the stomach due to cancer. This operation was done to postpone death from starvation for a time. He had much pain and had been vomiting practically all of his food. He was helped for a few weeks, but the disease soon returned even more extensively than before the surgery. It again caused obstruction that threatened an early death. A large, hard, bulging cancer mass occupied the upper abdomen involving the liver and the vomiting became worse than ever. Emaciation, cachexia, and weakness rapidly developed. This was the condition August 20th, 1926, at the time his physician, Dr. Harrison, brought him to Dr. Koch and the Glyoxylide was given.
Following this Treatment there was a rather rapid recovery. In from six to nine months, the large cancer masses were absorbed, the stomach healed, and perfect health was established except for the fact that the stomach is smaller than normal and with less capacity. He remained well up to the time of his death, over a quarter century later when he died, just a few years before his 100th birthday.
As will be seen from the pathologist’s examination of the tissue, this was the type of cancer that spreads far and quickly, metastasizing early. It is observed from the pathologist’s report also that only a part was removed and examined, so the great bulk of the growth must have remained in the stomach wall and in positions in the abdomen where removal was impossible. (Plate 11)
PLATE 11. This is a pathological laboratory report of the Methodist Hospital in Fort Wayne, Indiana, regarding the Case of Wesley Roebuck, dated July 7, 1926. The diagnosis at the bottom indicates cancer of the stomach.

The hospital record here reproduced gives the interesting pathological details that should be studied to appreciate the seriousness of the case. (Plate 12)
PLATE 12. This is an operative report from the same Methodist Hospital in the Case of Wesley Roebuck with cancer of the stomach.
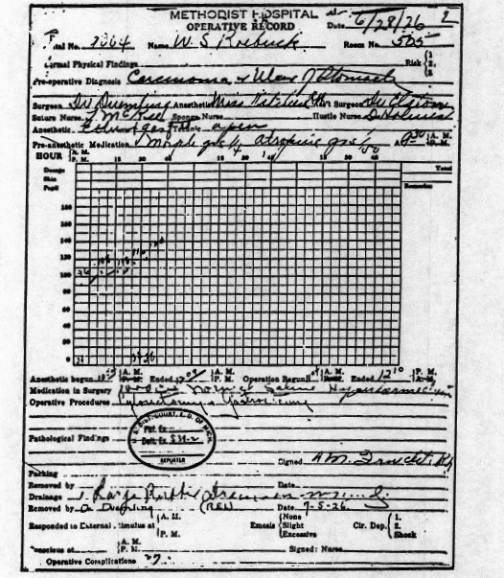
The recovery process came to completion in from six to nine months, and was characterized by reactions with aggravation of symptoms, fever, and general achiness for a few days at a time on three distinct occasions, including the twelfth and twenty-fourth week reaction periods. Between these reactions, improvement was rapidly progressive and recovery became complete.
TESTIMONY OF WESLEY ROEBUCK
(Note: The following is paraphrased from the Testimony given by Mr. Wesley Roebuck at the Koch Trial as found on pages 2845-2887 of the Official Court Record. The words below are those of Mr. Roebuck.)
“My name is Wesley S. Roebuck and I live about a mile and a half from the city of Fort Wayne, Indiana. I am in my eighty-second year and am a farmer. I have lived around Fort Wayne for forty-one years. When I was about thirty-five years old I had stomach trouble and it continued until I was about fifty. A few hours after I would eat I would get very sick and throw up my food. This continued for about fifteen years and I would work many a day without eating.
“During one winter the folks went to Florida and I discharged all the men except enough to keep the green house going and then I dieted myself. I baked my own bread out of whole wheat, soda, and buttermilk without any shortening, a little bit of sugar, and a spoonful of salt. My stomach got better and better and one day without giving any warning, it took a crazy spell and got well. Then I did not have any more stomach trouble until about 1925 or 1926.
“I did not move into town, but stayed on the farm and was elected Treasurer of Allen County; Treasurer pro tem of the City of Fort Wayne, which was the county seat of Allen County. I got along well for the first year and then along in the winter of 1926 my stomach began to go bad again. But this time it was different than any stomach trouble I had gone through. I could tell it was more serious. I got so that nothing would pass through my stomach and I would vomit everything that I ate.
PATHOLOGICAL LABORATORY
GROSS EXAMINATION: Tissue of stomach.
MICROSCOPIC EXAMINATION: Small alveoli combined with a diffuse growth of atypical proliferating epithelium from the structural picture of this neoplasm. The epithelial cells are generally polyhedral or round in shape, with large hyperchromatic nuclei. One portion is necrotic —a superficial ulceration. This may be classified, as the diffuse type of gastric carcinoma. I am unable to determine this point exactly as it is necessary to know something of the gross appearance. If there were extensive involvement of the wall, this would be the correct interpretation. If the growth were sharply defined, rounded and ulcerating, it would by placed with the circumscribed types of carcinoma simplex.
This type is always infiltrating and early invades the lymph nodes with wide—spread metastases.
DIAGNOSIS: Carcinoma of the stomach. (Type dependent upon the gross pathological anatomy.)
“I went to Dr. Duemling and was sent to the Methodist Hospital in Fort Wayne. After X-rays they operated on me. I was there about five weeks. I was all right for about six months and then the stomach trouble came back as it had the first time. It hurt so much that I could not eat anything and would always throw up if I tried to eat. Finally my daughter and Dr. Harrison of Butler, Indiana, took me to Detroit to see Dr. Koch. I had not known Dr. Koch before that.
“Dr. Koch examined me and gave me specific directions as to how to prepare for the Treatment. I went home and followed them to the letter. In about ten days, he gave me an injection. Then I went back home again. The first thing that happened was that I wanted something to eat. I was desperately hungry.
“I took to eating and in about five or six weeks, I had gained my original weight which was my usual weight—around 120 pounds. I was down to 105 pounds before I took sick. I was comfortably up and about almost right away. I kept at my business and did not hardly know I had a stomach. I had another Treatment four or five years later, but just for general condition, not because I needed it. I have not had any recurrence of this stomach trouble since then.”
A DISCUSSION OF THE REBUTTAL ATTEMPTED IN THE ROEBUCK CASE
The rebuttal in the Roebuck Case was the “opinion” that the operation might have removed all the growth and cured him. This “opinion” the witness based upon his idea that 4% of cases of cancer of the stomach can be cured by operation. He did not state whether or not he considered the fact that only the very early cases of the types that do not infiltrate early or widely, and are discovered by accident while doing some abdominal operation, and before cancer symptoms call for the operation, was in his mind when he gave that percentage. The consensus of opinion we learn from the authoritative writings and discussions with physicians of experience is that the growth must all be removed, and it is too late to do so after symptoms of cancer call for the operation.
The facts in this case, however, show that the growth was not all removed. The pathologist shows this when discussing the tissue from which he made the tissue slide. He states in his report here reproduced, “I am unable to determine this point exactly since it is necessary to know something of the gross appearance.” Thus, he shows that the whole growth was not removed to give him the gross appearance for his diagnosis, but only some “Tissue of the Stomach” as the “Gross Examination” reveals. If this pathologist had received a part of the stomach wall, which should be removed with plenty of healthy appearing tissue about it, he would have had the gross appearance and would never have made the comments present in his report. He would have before him enough growth, to answer all the questions made in his report.
He would have had the whole growth, could describe and study the gross appearance and would know how extensively the wall was involved.
This was, therefore, not a removal of the growth but a patch-up or palliative operation that secured a temporary relief from the obstruction. But, the disease was not all removed, since it was only a few months before it had progressed to a worse state than when first operated. All the symptoms returned as the facts show and besides an enormous growth sprang up, which could easily be seen to bulge and was easily felt to bulge outwardly, and to be fixed deep within the abdomen, and to involve the liver and surrounding structures. The renewed obstruction with its vomiting, pains that were worse than ever, and the cachexia that goes with far advanced cancer, are revealed in the facts in this case and these contradict the “opinion” of the Government witness.
The most important fact presented here, and one, which the Government could not even attempt to rebut, is the fact that recovery went hand in hand with the cyclic reactions that characterize the recovery from cancer under the Koch Treatment. The most important of these were the reactions soon after the Treatment, and those of the twelfth and of the twenty-fourth week. This recovery process is unique to the Koch Treatment and denies the “opinion” of the witness.
Inoperable, Far Advanced Carcinoma of the Stomach
THE CASE OF WILLIAM J. SCHULTZ
Introductory Remarks
The defense in this trial was well aware of the great distance a Government “opinion” witness, posing as an expert, will deviate from the truth in order to discredit the defense Testimony. Thus in several of the rebuttals, it was stated that the biopsy might have removed the entire growth, even though the facts showed this was not true nor possible. Here we present a case of far advanced cancer of the stomach, easily diagnosticated correctly by the physical examination and history, confirmed by the X-ray, and again confirmed by thorough exploratory operation by the Mayo Clinic experts, but no biopsy was taken because such procedure was not necessary for a complete perfect diagnosis. Not one bit of tissue was removed, so this case was presented to eliminate the rebuttal trickery just mentioned.
The case just previously detailed is one in which the biopsy diagnosis predicted the inadequacy of surgery, which was actually admitted in the record by the surgeons. The case to be described now had reached the terminal stage with its marked cachexia and enormous wide-spread cancer development, which had destroyed over half of the stomach wall, and spread to other organs, and up along the large blood vessels leading into the chest. Obviously biopsy was not needed as an aid to diagnose in such a case. Here all the developments that biopsy predicts for the disease, as it reaches fatality, had already taken place and were well established at the time the exploration was made at the Mayo Clinic in May 1941.
Two weeks before this exploration was made, the X-ray examination (May 12, 1941) gave an accurate picture of the destruction of the stomach wall. (Plate 13) This was the first radiograph that showed any stomach lesion. Pictures made in 1940, showed no lesion whatever. The type of cancer present, therefore, was exceedingly malignant and grew and spread rapidly.
PLATE 13. This X-ray of the stomach of William Schultz was made on May 12, 1941, showing accurately the destruction of the stomach wall as a result of far advanced cancer.
After being sent home from the Mayo Clinic, as a far advanced, hopeless, inoperable case of cancer of the stomach with metastases along the aorta, and with involvement of the surrounding structures and pancreas, he continued to decline rapidly and cachexia became extreme. Finally he was taken to Dr. Mantor of Sidney, Nebraska. He could not walk without help. He was given an injection of Glyoxylide and the trend of the disease was reversed. In six months, he had regained much of his natural vigor and was able to do considerable work. The following year, he did the farm work and husked hundreds of bushels of corn. X-ray made April 5th, 1943, at Tyler Clinic (Plate 14) showed about 75% improvement. His health was improving at this time. It is possible the defect remaining was due to scar tissue, which replaced the cancer tissue that was absorbed, but which was not yet replaced with normal stomach tissue. His health remained well and on June 15, 1944, a further X-ray was made at the Roche Hospital, Sidney, Nebraska. This shows a normal stomach. The deformities have disappeared and the stomach behaved normally ever since. (Plate 15) (Plate 16)
PLATE 14. This X-ray of the stomach of William Schultz was made on April 5, 1943, showing 75 percent improvement in the cancerous condition.
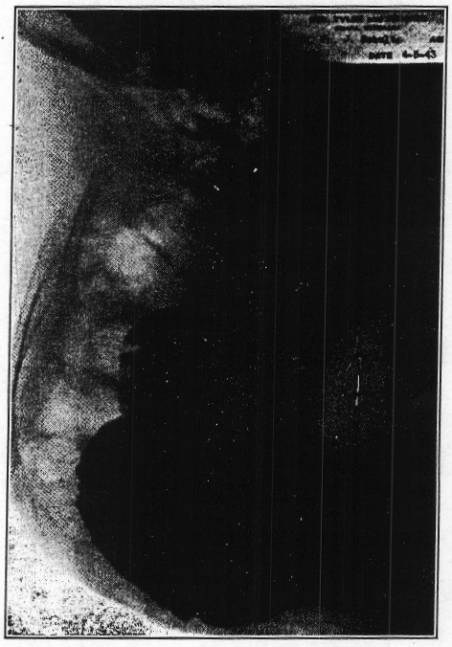
PLATE 15. This X-ray of the stomach of William Schultz was made on June 15, 1944, showing a normal stomach, after the Koch Treatment
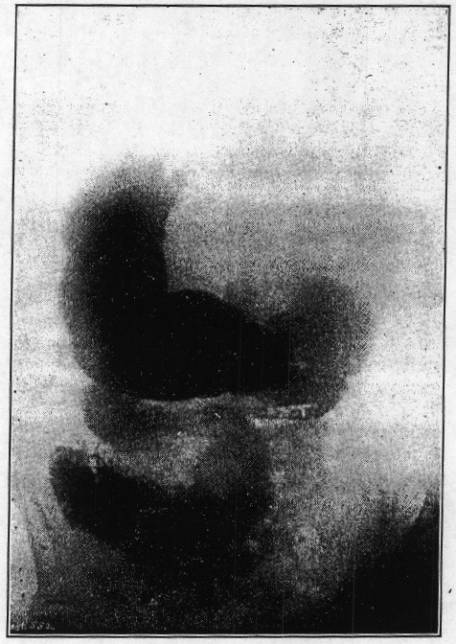
PLATE 16. This is a reproduction of the surgical card from the Mayo Clinic, showing that William Schultz was afflicted with cancer of the stomach, which was so far advanced that it was inoperable.
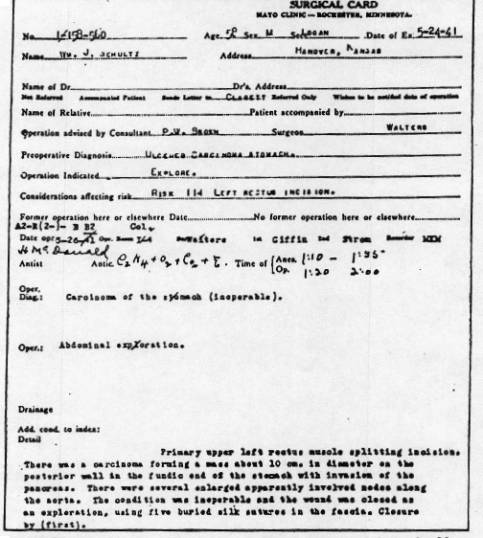
These two cases illustrate that very far advanced cases of cancer of the stomach that had no hope from other methods, actually secured permanent recoveries after a few Treatments of Glyoxylide.
Dr. Mantor gives a brief history of the case as follows and Mr. Schultz’ Testimony is also presented.
PARAPHRASE OF THE TESTIMONY OF DR. H. E. MANTOR
“William J. Schultz was brought up to see me by some of his friends.
“He was a pretty sick man. I sent him to a private nursing home. He said that he had had an exploratory operation at Mayo’s a few weeks before that he was in an exhausted state, weak, depressed, anemic, and his color was extremely bad.
“I did a crenation test, and his red cells did not crenate in a one percent salt solution. On physical examination, I found on his abdomen a linear scar of recent date, and he still had a dressing on it, and on palpitation, I could feel a massive induration in the epigastrium. The mass appeared to be in the stomach. Not only could you palpate it, but also you could see it protruding very plainly when he was lying down.
“He said he had had stomach trouble for about a year and a half, progressively worse. He took some treatments in some clinic in Kansas for a supposed gastric ulcer, but he had no benefit from it. Dr. Hurtig, his local physician, sent him to Drs. Tyler and Simonds, leading roentgenologists of Omaha, and he was given a diagnosis there of cancer. Dr. Hurtig told him he had best go to Rochester. He was operated on in the latter part of May, (Plate 17) and he came to me in June. I gave him Glyoxylide on the 16th of June.
PLATE 17. This is a letter from the Mayo Clinic to Dr. Mantor, describing the fatal condition of William Schultz before the Koch Treatment was administered.

“He went home and came back to me the ninth week. He told me he was doing fine and suggested another injection. I said, ‘No, you are doing fine, it’s too early.’ He had gained in weight, color improved, was more active. On examination of his abdomen, I could not palpate any induration whatever. The tumefaction had disappeared.
“The twelfth week I gave him another injection of Glyoxylide. At that time, he showed still further gain in weight; he was stronger, and more active. He was working some, and his complexion had cleared up nicely. In walking down the street with me, he could out walk me without getting out of breath. I didn’t see him for two years. He was in fine condition, and told me he was doing a great deal of farm work. I examined him in my office this morning. He seems to be in a very normal condition for his age. His skin was alive and flexible, and different to what we find in a toxic condition. It is a little characteristic that means a lot to a doctor in examination. The skin on his body was a nice texture and color.”
TESTIMONY OF WILLIAM SCHULTZ
(Note: The following is paraphrased from the Testimony given by Mr. William J. Schultz at the Koch Trial as found in the, Official Court Record. The words below are those of Mr. Schultz.)
“I live in Hanover, Kansas. I farmed for two years, and then I sold out and moved to town. Now I deliver ice. In 1940 or 1941, I had some sort of trouble. I didn’t know what it was. I went to Halstead two or three times in that winter, but they did me more harm than good. Then in May, I went to Mayo Brothers. I had been troubled for about a year before I went to Mayo’s with pains in my stomach, day and night. My normal weight was 155 or 150 pounds, and I had gone down to 120. I had had to give up my farm on account of these ailments.
“Dr. Hurtig, in Hanover, sent me to Omaha, and had Dr. Tyler take pictures of my stomach. My stomach was very swollen, and Dr. Hurtig talked me into going to Mayo’s. Two weeks after the operation at Mayo’s, I was in awful pain, my stomach was swollen, and I was vomiting.
I went to see Dr. Mantor, and he put me in a nursing home for three days, put me on a diet, and gave me an injection in the arm. It didn’t take long after I got back to Hanover before I began to feel better. I got to feeling so good that I went to work, farming 170 acres and taking care of forty-five head of cattle with the help of my brother. I feel fine now and can eat anything. I have had three injections in all, about a year apart.
“Dr. Hurtig took me up to Dr. Tyler’s again about a year ago to have more pictures taken of my stomach. Dr. Hurtig came over and asked me to go, and I did it just to accommodate him. I didn’t pay for the pictures, and I was not paid for going.”
The pictures just mentioned were paid for by the Food and Drug Department to ascertain the patient’s progress. The information gained from comparing the first set of pictures taken at the Tyler Clinic and the second set, under discussion, showed the stomach had recovered about 75% and is so recorded on the Tyler Clinic cards in the hands of the Federal Trade Commission, at present, as exhibits. However, this improvement after the Koch Treatment was not reported by the Food and Drug Department to the American people, who paid for the information. It was suppressed and instead an attempt was made to discredit the value of Glyoxylide in such a cancer condition as Schultz’s.
ANALYSIS OF THE REBUTTAL OF THE WILLIAM SCHULTZ CASE ATTEMPTED
BY DR. BELL
The rebuttal in this case was the “opinion” offered by Dr. Bell, of the Hertzler Clinic, a possible rival of the Mayo Clinic. He offered the “opinion” that the disease, which the Mayo experts actually observed when they opened the abdomen, and examined the stomach, the pancreas, and the lymphatic glands along the aorta, and actually found to be a far advanced carcinoma of the stomach, was only a “typical picture of gastric ulcer.”
Dr. Bell explained the lesions he never saw, as widespread inflammation due to infection. In other words, that Mayo’s doesn’t know the first thing about making a diagnosis, and to be in harmony with this wrong conclusion, Schultz would have to be lying in bed tightened up with pain, too tender to be touched, the abdomen hard as a board, with high fever, and passing out from the toxemia of the infection. The facts show that Schultz never was in such a condition, and hence, Dr. Bell’s “imagined” diagnosis is not supported by the facts, for that is exactly the condition he would be in, if Bell’s “opinions” were correct. Thus, neither the symptoms Schultz presented, nor the facts observed by the Mayo experts, support the “fancies” of Dr. Bell.
It must be recalled that Dr. Collar, the surgeon of the University of Michigan Hospital, testified in the first trial that he could and did consistently diagnose cancer and other disease that occur within the abdomen correctly with 100% accuracy by exploratory operation and his diagnoses were proven correct by microscopic check-up. Other surgeons are known to be correct over a period of twenty-five years through similar check-up. The “opinion” given by Dr. Bell is therefore quite a shock.
The Mayo experts did this exploratory to make a thorough and correct diagnosis. If there were a shadow of a doubt, they would have made a biopsy for a scientific, as well as, a moral obligation. If they had found inflammation, they would have recorded it and identified the germ that was responsible, so as to be able to give appropriate treatment. But in a clear-cut case of cancer, which carried no complicating factors, the biopsy was not needed and to inflict injury, which added nothing to the certainty of the diagnosis, is simply bad practice for which Mayo’s do not have the reputation.
Dr. Bell also gave the “opinion” that the diet, which Dr. Mantor had Schultz follow, was responsible for the cure. Here again Bell is contradicted by the fact that the diet used with the Koch Treatment is a high-roughage diet, which ulcer cases do not tolerate. The whole theory and practice of gastric ulcer treatment forbids the Koch Diet in gastric ulcer, but relies upon a soft bland diet, and the use of alkalies instead of the acids of the Koch Diet. There is no scientific or clinical basis for Dr. Bell’s claim therefore. The very opposite is true.
Let us, to help Dr. Bell, admit that the high acid, and high-roughage diet Schultz followed did coat over and soothe the ulcer in the stomach. But, how on earth would it get to the pancreas and the lymph glands, and along the aorta to soothe them? Here we see once again the travesty of permitting an “expert” to pass judgment on something he never saw, when as the other witnesses for the Government admitted, you cannot make a diagnosis without observing the patient yourself, or you will not know what you are talking about. Dr. Bell could not be quite so uninformed as not to know this.
THE CASE OF MRS. CHARLES TRAPP
Far Advanced Cancer of the Cervix Uteri Cured Over Twenty-five Years Ago,
Gave Birth to Healthy Children, Perfect Health Still Remains.
Introductory Statement and Testimony Data
THIS IS A CASE of inoperable cancer of the cervix uteri in a young woman of thirty-one years who was treated with Glyoxylide in August 1923, and made a perfect recovery, remaining well for a quarter of a century. She also gave birth to four healthy children after being cured. The mother and the children all remain well. This woman had been married several years and was unable to bear a child. One abortion occurred a few years before cancer began to show symptoms of attacking the uterus. There had been profuse irregular bleeding, mucopurulent discharge, for a year or more and then pain and irritable bladder with reduced capacity. A biopsy was made by Dr. L. N. Tupper and the laboratory report is reproduced. (Plate18)
PLATE 18. This document shows the laboratory report in the Case of Mrs. Charles Trapp, made on August 1, 1923, indicating cancer of the Uterus. After taking the Koch Treatment, Mrs. Trapp not only recovered, but also gave birth to four healthy children during the next twenty-five years.

“The patient on examination was found to present a massive, far advanced, cancerous involvement of the cervix uteri, the body of the uterus, and adnexa on the right side. The cancer mass was fixed, and “froze” the involved tissues into one immovable hard mass, which obliterated all normal contours and was palpable above the pubes one-third of the way to the umbilicus. Thus, the disease was extensive and entirely inoperable. Bleeding was frequent and profuse.
“Two injections of Glyoxylide were given, one on August 7th and one on August 21st, 1923. The recovery was rather rapid, with the reaction phases every three weeks until recovery was completed within thirty-six weeks after the Treatments were given.
“At this time there was a well-healed, freely movable uterus, and normal adjacent tissues, but there was some deficit in the cervix and uterus structure, where full restoration of destroyed tissue had not yet been completed. However, in some six months the uterus was quite well reconstructed. Pregnancy took place the next year and a normal child was born after a normal term. Three other normal children were born at subsequent periods. There was no return of malignant involvement and the patient and her children remain in good health, these twenty-five years.
“This case ought to illustrate the permanency and completeness of recovery and the restoration of tissues and function, also the resistance to cancer that is established. Thus, the trauma of four pregnancies failed to cause a return of the disease, so a true recovery is actually established.
“This Case of Mrs. Trapp offered facts, which could not be rebutted. The slide carrying the biopsy specimen was held at the Owen Clinical Laboratory until shortly before the first trial, when a defense attorney, Mr. Long, went to the laboratory and asked if they would produce the slide. The answer was that the slide was on file until a few days ago when Federal investigators asked for it, since which time it was no longer to be found.” The reader can draw his own conclusion.
However, the original biopsy report was admitted into evidence after being identified through its signature of Dr. Robert Owen, the pathologist. The identification was established by handwriting experts. Thus, the diagnosis could not be successfully rebutted. The case was also presented before the Federal Trade Commission, but the Testimony was not allowed. The Testimony shows that the specimen removed by Dr. Tupper was placed in a small bottle, which the husband brought home and which the brother-in-law took from the home to the Owen Clinical Laboratory. Since this bottle was not given exactly the same description by both of these gentlemen, when testifying more than twenty years after they had seen it, the trial examiner for the Federal Trade Commission would not allow the Testimony to be presented.
However, it was not the bottle that was the subject of the biopsy; it was the specimen carried in the bottle and removed by Dr. Tupper and examined by Dr. Robert Owen.
Here is an instance of a cure of cancer of the uterus following the Koch Treatment, knowledge of which should be of the greatest value to cancer sufferers throughout the world. But this is denied public record by the Federal Trade Commission trial examiner. Thus, one can see what the attitude of the bureaucrats is, in a matter of such great importance where the public welfare is concerned. More flagrant instances will also appear in this writing.
Mrs. T. showing three of her four children born after recovery. The fourth was born one year later.

Cancer of the Uterine Cervix
THE CASE OF MRS. LAURA JANE JOHNSON
Introductory Remarks
Another case of cancer of the cervix uteri is that of Mrs. Johnson, age thirty-two, when entering the Koch Clinic, November 25, 1931. Her diagnostic and surgical history, are given by the hospital records. She made a complete recovery following the Koch Treatment and remains well now after seventeen years.
This was a terminal case, in the very last stage, where cachexia was well established and the cancer tissue had invaded the whole pelvis “freezing” the tissues into a solid structure with loss of the natural anatomical contours, and landmarks. The Microscopic Diagnosis was: “Well developed Medullary Carcinoma,” Surgical Diagnosis, — ‘Advanced carcinoma of uterine cervix’. Examination showed the cancerous growth to have developed from deep in the pelvis to half way up to the umbilicus. The bladder wall was involved to a great extent and the bowel wall also, so that urinary difficulty and partial obstruction of the bowel resulted. (Plate 19)
PLATE 19. This final diagnosis of “Medullary carcinoma of cervix,” was made by the Highland Park General Hospital in 1928 in the Case of Laura Johnson.
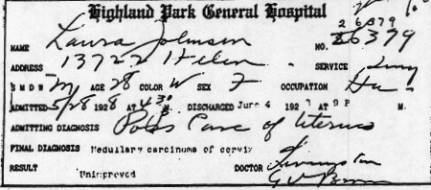
“Much of the cancerous growth was already gangrenous, causing putrid drainage, bleeding, etc. Certain cerebral symptoms suggested that the metastases had spread to the brain. At any rate, there were convulsions without the loss of consciousness. The patient was so weak she had to be almost carried into the office. She had lost much weight, the tissues were waterlogged, (transparent), and the typical yellow tint to eyes and skin showed advanced hemolysis. She was in the last stage of the disease.
“Before the disease reached this stage of advancement, attempts were made to retard its progress and to reduce hemorrhage by cautery of the cervical necrotic area and by tying off some of the blood vessels that nourished the uterus. Delay might have been secured by this means for a few months. However, the disease is often markedly stimulated into greater malignancy and widespread metastases by surgical measures that fall short of complete removal. Perhaps the great advancement of the disease at the time of the Koch Treatment is thus explained.”
This case illustrates very well that recovery can take place in spite of the stimulation caused by anesthetics, cautery, and surgical manipulations, the bad effects of which are so well known and recorded by experts, as seen in the following quotations:
“Statistics favor the conclusion that operation, on the whole, shortens life in recurrent cases, although sometimes rendering it more tolerable. Handley’s recurrent cases lived 29.6 months, while in the above series, the duration of life of un-operated cases was 27, 29, 34, and 48 months respectively. This conclusion is strengthened by theoretical considerations, as well as, by observations on the rapid course of many recurrent cases. It is clearly proved in many instances by the increasing anaplasia exhibited in the structure of recurrent tumors.”
“In estimating the economic importance of the surgical treatment of mammary cancer, there must be charged up the cost of acquiring surgical skill, and the deplorable conditions following local recurrence. There can be no doubt that operation shortens life and aggravates the terminal suffering, in the great majority of recurrent cases.” Ewing, pages, 597-598.
“There can be little doubt that the rough manipulation of cellular tumors, in the preparation of the patient and in the excision of the growth, widens the field of infection by forcing cells through vessels and tissue spaces.” Ewing, page, 73.
“Arising from remnants of the original growth recurrence is usually prompt, multiple, in the line of incision or near by, and of the same type as the original growth or more malignant.” Ewing, pages, 73 and 74.
“Injury, whether a bruise or massage, to a pre-existing cancer, has been associated with an apparently extraordinary dissemination of the disease due to it. Aspiration of breast lumps for diagnosis falls into this category. . . Aspiration biopsy should be given up entirely.” Pullen, page, 245.
“Rapid and progressive multiplication of tumor-cells without notable intermission or hindrance is characteristic of most highly malignant neoplasm.” Ewing, page, 44.
“Cancer of the cervix is found inoperable the first time it is discovered at the first examination. The MORTALITY from uterine cancer is very high. Cullen states that of cervical cases, 50% are inoperable when first seen.” 1% are permanently cured; 8% live five years, (of operable cases).” Ewing, page, 620.
“Gaylord offers experimental evidence to show that prolonged anesthesia and hemorrhage reduce the resistance to cancer.” Ewing, page, 597.
“The rapid progress of the disease is illustrated by Mackinrodt’s observations who found the disease beyond the uterus in half of 18 cases examined within four weeks after the earliest definite symptoms. After the second month, 20 % of his cases were inoperable; after six months, 40%.” Ewing, page, 616.
“In cervical carcinoma the early involvement of the parametrium and its nodes was fully demonstrated by Kundrat who in 160 cases found this structure involved in 55%, while Lamaris and Kermanner saw such extensions in 57 1/2; Baisch in 36% and Schauta in 64 %.” Ewing, page, 617.
“The clinical course of the advanced disease is dominated by the secondary invasion of neighboring organs.” Ewing, page, 619.
“Characteristic cachexia in uterine cancer develops in the terminal stages of the generalized disease, but when the lesion is localized in the pelvis, cachexia is missing.”
In view of the foregoing established knowledge, the reviewers conclude that the advanced stage of cachexia, which existed at the time of the Koch Treatment, showed conclusively that the terminal stage of the disease had been reached and that death was not far off.
DATA FROM DR. KOCH’S TESTIMONY
“The first dose of Glyoxylide was given November 25, 1931. A reaction took place in twenty-four hours, with chills, fever, and general achiness, and a slight erythematous rash. After about ten days a definite improvement developed. This improvement was progressive with reactions intervening at three-week intervals. The reactions were like the first showing chills, fever, and a general malaise and achiness, but grew less intense each time, and were of shorter duration.
“The periods between reactions showed more improvement as time went on, until full health was restored. This took about a year, and the gain in weight went from 130 pounds to 180 of good healthy solid flesh. The cancerous extensions throughout the pelvis steadily absorbed leaving the parts normal, but the uterus itself was not completely restored to a normal shape until two years had passed. An examination made in April 1946, revealed a normal pelvic and uterine structure and her health remains perfect. There is no recurrence of the disease.”
THE TESTIMONY OF LAURA JOHNSON
(Note: .The following is paraphrased from the Testimony given by Mrs. Laura Johnson at the Koch Trial as found on pages 5931 of the Official Court Record.)
Mrs. Laura Jane Johnson resided in Port Huron when she testified at the first trial and in Sacramento, California, when she testified at the second trial. She lived in Detroit, Michigan, at the time of her illness and when she first received the Koch Treatment.
“About 1928, she experienced bad pains in the lower abdomen and found it difficult to walk. She was twenty-eight years old at the time. She then went to see Dr. Livingstone, accompanied by a friend. She didn’t feel any better after she left Dr. Livingstone. Her second doctor was Dr. Van Amber Brown, who was in a clinic on Woodward Avenue in Detroit. Dr. Brown sent her to the Highland Park General Hospital on May 28, 1928. The hospital record is Exhibit No. 130 in the first trial. It reads in part: “She was advised that these findings were suspicious of a probable malignancy of the uterus and that prompt surgical treatment in any event was indicated.”
“The pathology report made by Dr. Brown and dated May 29, 1938 reads in part:
“Well developed Medullary carcinoma.” An extirpation by cautery of the cervical growth was made on May 29, 1928. She was discharged from the hospital on June 4, 1928, with the tumor removed. She returned to the hospital on June 13, 1928, because of a severe hemorrhage, which followed the operation. The report on June 14, 1928, gives the following: “Diagnosis: Advanced carcinoma of the uterine cervix.” Pathology report: “chronic endocervicitis erosion.”
“Mrs. Johnson left the hospital for the second time on July 1, 1928, but felt no better. She wasn’t comfortable at any time. She went back to her native state, North Dakota, in July 1929. During all this time, she saw Dr. Brown three or four times a week. She had no X-ray or radium although it had been advised. She seemed improved for a short time after returning from North Dakota to Detroit. Suddenly an attack with severe pain took hold of her on the way to taking her children to school. She then went to see Dr. Rose who had taken Dr. Brown’s place. He examined her. She saw him for about two months. She didn’t feel any better, but she had no hemorrhage. Next she went to see Dr. Koch in November 1929. Dr. Koch examined her. She told him her history and he put her on a diet and then gave her the Treatment. Her husband was with her.
“Mrs. Johnson began to feel improvement in about three or four weeks. She had been in pain and mostly in bed for a year and a half since she left the hospital and before she received the Koch Treatment. A few weeks after Dr. Koch treated her she could get around the house and do a few things. She had reactions which acted like a “grippe” but they decreased in intensity each time as she continued to get well.
“She received a second injection of the Koch Treatment six months after the first. This was given by Dr. Stiers. Her recovery became even more rapid. The third, was six months after the second and was administered by Dr. Koch, personally. She said she didn’t need it, but her husband insisted. Mrs. Johnson testifies that she now feels fine and has never had a return of pain or symptoms, such as she experienced before she took the Koch Treatment. She has had no other medical treatment and testified in 1946 as to her good health. She has had four children; one died in childbirth. Her cancer case had been biopsied and neutral hospitals made the diagnosis. She has had no recurrence even after fifteen years of enjoying fine health.
ATTEMPT AT REBUTTAL
In the first criminal trial, the Government failed to produce any rebuttal Testimony, fact or “opinion,” and the case stood unchallenged, it is also evident from the authoritative quotations just given, that “opinion” Testimony could not possibly stand a show of contradicting the facts presented by this case.
It was admitted throughout all trials, by various Government “opinion” witnesses that it is necessary to personally observe and examine a patient, before a diagnosis can be made. Thus, the “opinion” Testimony given in the various cases is acknowledged by the witnesses that give it to be worthless, it does seem strange that “opinions” of fairly inexperienced and little known physicians, who have never seen the patient they are testifying about and never observed the manifestations of the diseases they are testifying about, should be permitted to be given before a jury; or to a commission, for the purpose of discrediting the diagnosis of such well-known experts of such broad experience, as carry the responsibility for the Mayo Clinic, the University of Michigan Hospital, the Henry Ford Hospital or of Dr. Kannel of Fort Wayne, Indiana. This is especially true when the opinions recorded in the hospital records, are based upon careful study and examination of the case during the presence of the disease, when all of the factors that constitute the disease are plainly before the experts. In other words, how could a second-rater, who has never seen the patient, know more about the diagnosis than the experts who studied the case and made examinations of the diseased conditions that actually existed, right when they existed?
This is all the more evident when all experts, including the second-raters, claim they must first see the patient and examine, personally, to arrive at an accurate diagnosis. The New Deal Government, therefore, was not giving the jury, the commission, the suffering public, or the Treatment they tried to condemn, anything like a square deal. Still, at the second trial, Dr. Wirth hazarded an “opinion” that the cure was due to the cautery and starvation ligature to some of the blood vessels that feed the uterus. But this “opinion” is not valid, since the disease was only retarded for a period, and continued to spread to a richer blood supply when it burst forth with great vigor and spread throughout the pelvis and to distant parts. Thus, the facts defeat Wirth’s “opinion.” It must be stated too, that had the blood supply been completely severed from the affected parts so as to actually starve the cancer, the patient would have died of gangrene long before she ever saw Dr. Koch.
LYMPHOSARCOMA
Lymphocytic Cell Type
THE CASE OF MRS. MERVIN SPARLING
The most rapidly fatal type of cancer is the lymphosarcoma of the lymphocytic type. Such cases are inoperable. They may give a brief favorable response to irradiation, but in a short time the disease returns with violence and kills. It is recognized that irradiation does not lengthen life one day in this disease. Lymphosarcoma of the lymphocytic type is fatal in six weeks to three months as a rule. Cachexia does not set in until the terminal phase and when it does show up, one can count on an early fatality. The consensus of authoritative opinion is quoted herewith, to show the sort of disease with which we are dealing.
“Yet it was one of the most malignant diseases, resisting attempts to extirpation, and proving a veritable ‘noli me tangere'” (‘touch me not’). Ewing, page, 422.
“The usual course is progressive, and fatal within a few months. Wide extensions are observed chiefly with more prolonged course. After local treatment, extirpation, internal use of arsenic, or application of X-ray, the disease has often appeared to be arrested only to recur after a brief period.” Ewing, page, 423.
“The tumors arise in a chain of lymph nodes or in a localized lymphatic structure, and rapidly produce bulky growths, which obliterate the outlines of the separate nodes, infiltrate surrounding tissues, and tend to result in necrosis, and ulceration of skin and mucous membrane. The more rapid cases are fatal; while the growth is chiefly local, but widespread extensions and metastases are commonly observed. Fever is often a prominent symptom, but anemia and cachexia may not appear until toward the end of the disease. In comparing cases of lymphosarcoma with those suffering from Hodgkin’s disease, it may often be noted that the former do not appear to be very ill until shortly before death, while the typical Hodgkin’s case is feeble, emaciated, and cachectic for a long period.” Ewing, pages, 422-423.
“The disease, which is invariably fatal, may involve the entire lymphoid apparatus of the body, not only the lymph nodes, but the lymphoid tissue in the pharynx (tonsils, etc.), gastro-intestinal canal, spleen, bone-marrow, liver, and other organs. Often the lesions are much more marked in one position than another, and indeed the disease appears to begin in one part of the lymphatic system and spread slowly from one group of glands to another, so that we may distinguish a cervical, mediastinal, and abdominal form, the glandular enlargement in these regions dwarfing that observed elsewhere.” Body, page, 809.
The present case is one of the rapidly fatal type, which had gone into the terminal stage of cachexia and she was failing rapidly at the time she received her Treatment with Glyoxylide.
The history shows that there was some sensitivity of the right side of the neck to cold air in 1943. Boils developed under the axilla on both sides, and sulfa drugs and frequent lancing did not help.
However, an autogenous vaccine did help and recovery from this was apparently complete.
In September 1944, the neck became stiff and enlarged on the right side forming a tumor that was hard and attached and rapidly infiltrated into and beneath the neck muscles and the tonsilar region within the throat. Other tumors quickly appeared in the axilla and the groins. Biopsy was made removing not more than a third of the projecting parts of the growth in the neck, on October 14th, 1944, by Dr. J. M. Jones of Bay City, Michigan. The laboratory report by a very reliable pathologist is reproduced. (Plate 20)
PLATE 20. This is a reproduction of the laboratory report in the Case of Mrs. Sparling. Note the diagnosis: “Lymphosarcoma.”
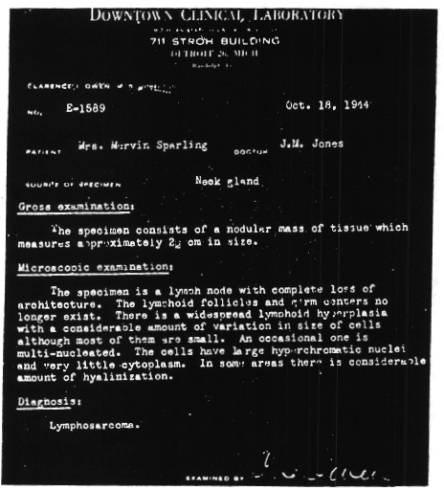
After this biopsy was made the growth developed very rapidly.
“Physical examination made by Dr. Koch on October 27th, 1944 and reported in his Testimony, revealed considerable cachexia, the lemon, yellow color of the skin of profound hemolysis, emaciation, and rapidly developing weakness.
“The neck showed swelling inside in the tonsilar region of the right side and a hard fixed infiltration tumefaction involving all the tissues on the outside of the neck from the ear to behind the clavicle. It bulged out forming quite a tumor and reached from the spine behind to the larynx in front. The scar showed where the biopsy was taken and an area of central necrosis had developed at that point. Both sides of the neck showed single, gland involvement and both axilla and groins, especially the right groin, showed the same type of tumefaction. A large, hard, fixed mass was felt in the epigastric region, like the top of a man’s head. It had grown up from deep within the abdomen and could be felt to bulge quite definitely.
“The injection of Glyoxylide was given intramuscularly October 27th. There was a definite improvement in a week, both in the size of the tumors and in the degree of the cachexia. In six months, all tumor tissue had been absorbed, so far as examination could determine, and she appeared to be entirely well. She had a few severe reactions, particularly during the third, sixth, ninth, and twelfth weeks, and at the twenty-fourth, and thirty-sixth week. Chills, fever, general aches, and soreness, of the affected parts and areas where tumefactions had disappeared, characterized these reactions. Her recovery appears to be complete.”
From the Testimony of Dr. Jones, one of the best and most experienced surgeons in Michigan, it is evident that the disease was not removable surgically, and that it still existed in its rapidly growing form when the Koch Treatment was given. The cure must, therefore, be credited to the Koch Treatment, and not to the removal of the biopsy specimen, as the rebuttal habitually claims no matter how contrary to the facts, such a claim is proved to be.
PARAPHRASED FROM THE TESTIMONY OF DR. KOCH
“Mrs. Sparling is a young woman who became affected with lymphosarcoma of the violent type, the lymphocytic cell type of lymphosarcoma. I had the opportunity of observing her on October 27th, 1944. I found that on the right side of the neck there was a tumor that measured about two inches in width and two and three-quarter inches in length, and had projected out from the side of the neck, possibly an inch or so. There was an incision of the skin where the biopsy was made and there was an opening, some scab on the surface.
“Her nutrition was not good; she appeared to have lost weight. Her color was quite yellowish even at night, with the electric light, and her skin dry. The color indicated a blood destruction and a very toxic condition. The whites of her eyes were tinted a little towards yellow, also. The lymph gland enlargements were found not only in the neck, where the neoplastic tissue had infiltrated the muscle from the thyroid cartilage to the neck muscles posteriorly and from the ear above to the collarbone below, but they were also found in both axillae, in the groins, and in the abdomen. Here a large tumor mass that extended from the posterior abdominal wall to the anterior wall was fixed hard and almost bulging, and presented the dimensions of a man’s head.
“She was given an injection of the Glyoxylide and the result was an energetic recovery that took about six months to become complete. Recent examinations indicate the recovery to be complete. There is no evidence of the sickness existing now and her good health has returned, natural weight, etc. (Court Record: Pages 5680-5684.)
TESTIMONY OF MRS. MERVIN SPARLING
(Note: The following is paraphrased from the Testimony of Mrs. Marvin Sparling, at the Koch Trial as found on Pages 5684— 5695 of the Official Court Record. The words below are those of Mrs. Sparling.)
“I was ill in 1943. I had a soreness and stiffness in the right side of my neck. I could not stand wind in my ear. Riding in the car, I couldn’t stand a draft on my neck. That was in the early part of 1943. I consulted medical advice. I was told to rub camphorated oil on it. My condition did not improve.”
FURTHER DEVELOPMENTS OF ILLNESS
“I had masses of boils under each arm. I also consulted medical advice about that condition. They were lanced at different times, but they always returned. The boils appeared in April of 1943, and the doctor would lance them and I would go about, perhaps a week, and they would return and he would lance them again. The doctor who did this was Dr. Slattery in Bay City. They kept reappearing all summer. He gave me something to rub on them—I do not recall what it was—but along in the fall, they became much worse. He gave me a sulfa drug, which did not seem to do any good. I broke out all over and he had to quit giving it to me.
“Then he suggested I take X-ray treatments. I took one treatment and that did me no good, so I did not take any more.
“I then got to a state where I was in bed with agony with the boils under my arms, and so I called in another doctor and he took me to the hospital and lanced the boils and put gauze on so that they would drain, but they did not go away; they kept coming back. He gave me another kind of sulfa, other than what the previous doctor had given me and as long as I took the sulfa, they stayed away. But, as soon as I quit taking it, they reappeared.
“I then consulted further advice in that matter. This doctor’s name was Dr. Woodburn. He went to the army and I went to another doctor who was working with him, Dr. James Wilcox, and he made a serum and injected eight shots into my arm, which stopped the boils. The boils then went away.”
“Every time I swallowed, I could feel a growth inside my neck and the outside continued to be very stiff and it was enlarged.
“Sometime later I was bathing and I stepped on a rusty nail and tore my foot—and in a very short time trouble came— my ankle and foot started to swell, and I was very much afraid of blood poisoning, but I did not have blood poisoning. But, my neck flared up very much at that time; became much worse. I consulted medical advice about that, the doctor asked me to have my teeth X-rayed, which I did, and found nothing wrong with my teeth. This was an ear, eye, nose, and throat specialist, Dr. Hoyser. I told him there was something in there, that every time I swallowed, I could feel it (I refer to my throat) and the gland was noticeable, quite noticeable, at that time.
“He gave me some black salve to rub on twice a day until it disappeared. For two weeks I did that and it only aggravated it and made it grow very rapidly. After I put the black salve on for two weeks, I went back to him, but he was out of town, attending a convention in Chicago, so I went to a friend who was a doctor, Dr. H. C. Moore, and he suggested surgery.
“On October 14th, 1944, I had my neck operated on by Dr. J. M. Jones, of the Samaritan Hospital in Bay City. For two days it felt fine. At the beginning of the third day, it started to grow rapidly. I thought that it was the incision that was not healing and the day I left the hospital, which was the fourth day after I had it removed, the nurse put some drawing salve on it, thinking that it was not healing. She dressed it for me and I went home. After I got home it kept getting larger and paining, and it did not seem to be healing as it should, so I went back to the doctor who had suggested the surgery, to have it dressed. He sent me back to the doctor who did the surgery. He told me that he would not do anything for a few days. He put a clean dressing on and that is all.
“After that it continued to grow and to be very, very, painful and more or less a gripping sensation both inwardly and outwardly. I thought it was not healing properly and I put a hot application of boric acid on with the hot water bottle, which blistered it and made it worse.
“I then went back to the doctor. He did not do anything. The doctor I went to suggested deep therapy, but I did not have deep therapy. I came to Detroit to see Dr. Koch on October 24th, 1944, but I did not see Dr. Koch at that time. I talked to Dr. Richards and another doctor who was there from South America. I was put on a diet, a three-day diet, and I went back to Bay City. They recommended enemas twice a day. “I saw Dr. Koch, personally, on October the 27th, 1944, at eleven o’clock at night. Dr. Koch came to my home, gave me an examination, examined my stomach; in fact, he examined me all over and when he hit here (indicating), I knew there was something there, although I had not known that before. I could tell by the way it sounded that there was something hard there. He examined me all over and asked me a few questions about my weight and so on.
“At that time, Dr. Koch administered his Treatment. I observed results fifteen hours later. I received the shot after eleven o ‘clock. I am not sure, just exactly, but I know it was eleven o’clock when Dr. Koch arrived and the next day at two o’clock in the afternoon, I felt a relaxation in my neck and I started to run a slight temperature, and I had chills, a great many chills all night, and for about three weeks I had chills and a slight fever, and some aches in my legs and arms.
“The sore where I had burned myself with the boric acid, scabbed over and dropped off within about five days after Treatment. “The swelling in my neck gradually went down; every morning I could notice a difference in it. “I do not have any swelling in my neck now and I swallow freely without discomfort. I feel fine. I do my own housework and I assist in a ladies’ dress shop, in Bay City.”
Cancer of the Spleen
THE CASE OF BEVERLY GRAVES
This is a case of sarcoma of the spleen, in a young girl of six years that developed pain in the stomach and chest with rapid breathing, some diarrhea, bulging of the abdomen, and some fever. There was enlargement of the spleen and auxiliary and inguinal lymph glands. The child was taken to the hospital and the exploration was done by Dr. J. W. Kannel, whose description is given here along with the hospital record.
DATA FROM THE TESTIMONY OF DR. KANNEL
“This operation was performed in the Methodist Hospital. I found an enlarged spleen extending two inches below the ribs, and compressing the left lung, two-thirds of the lower part of that lung. The upper third was patent. That was the left lung. The ribs showed creasing or indentations in the spleen. It was irregular and hard. She was only sick, five days before I put her in the hospital and operated on her, because the progress of this case was so rapid.
“Her blood count the first day was 7,200 white cells, and on the twenty-third it was 16,700. We knew she had some very virulent disease there and we thought it was an abscess and when we got in there, we found it was not. The spleen is an organ that is a kind of reservoir to equalize the circulation of the blood and manufacture cells of blood. The normal, adult spleen is supposed to weigh one-half pound and occupy a position in the axillary line under the tenth and eleventh rib, so it couldn’t be very big in a child. It would be much smaller than that.
“The operation of June 1943, is known as an exploratory laparotomy. I did not remove anything or change the condition of any of the organs, but closed the abdomen. The operation was on June 24th, 1943, and on the seventh or eighth day, she was sent home. After the operation and examination, on the basis of my clinical findings and the history that I received, I made a final diagnosis of cancer of the spleen. I made this diagnosis because of the rapid increase of the white blood cells from 7,200, I think, to 16,700 on the 23rd, and on the 24th, just before the operation—and that is not in your record—it went up to 22,400. We immediately sent her to the operating room.
“There was a nodular condition of the spleen, irregular, with impressions of the ribs in it, and it was very hard. The normal condition of the spleen would be more soft, and be so small that it would not have projected down below the ribs nor compressed the lung. My first diagnosis, before we looked in, was enlarged spleen, possibly malignant. My final diagnosis was sarcoma of the spleen, made on June 24th, 1943. (Plate 21)
PLATE 21. This is a reproduction of the summary sheet from the Ft. Wayne Methodist Hospital in the Case of Beverly Graves, showing that the final diagnosis of her condition was cancer of the spleen.

“I later treated little Beverly in her home with a dose of Glyoxylide on July 2nd, 1943, eight days after the operation. She gradually improved and made a perfect recovery. She is now a well child and there has been a complete recovery of her splenic condition. She received no other treatment after my exploratory operation, my laparotomy, other than Glyoxylide. “I ascribe her recovery of that cancerous condition to Glyoxylide.”
TESTIMONY OF GEORGE CHARLES GRAVES
(Note: The following is paraphrased from the direct examination Testimony, given by George Charles Graves at the Koch Trial found on pages, 3820-3822, 1/2 of the Official Court Record. The words below are those of Mr. Graves.)
“My full name is George Charles Graves, and I live in Fort Wayne, Indiana. I am self-employed, being a dry cleaner.
“I am the father of Beverly Graves. I have been in the courtroom while Dr. Kannel testified to her case. I know Dr. Kannel and he is our family physician today.
“Beverly was 11 in 1943, and Dr. Kannel performed an operation on her at Methodist Hospital. After a period of time, she went back to school. Beverly goes to school and since last September has missed two or three days.
“I received a diagnosis from all three doctors. The other two doctors were Dr. Parker and Dr. McCoy. They attended the operation.
“As far as I know, my daughter is well today.”
TESTIMONY OF BEVERLY GRAVES
(Note: The following is paraphrased from the Testimony given by Beverly Silvan Graves at the Koch Trial as found on pages, 3847-3850 of the Official Court Record. The words below are those of little Beverly Graves.)
“My name is Beverly Silvan Graves, and I live on Maysville Road, Rural Route 9, Fort Wayne, Indiana. I go to school and am in the third grade. I missed today.
“I am nine years old. I went to school yesterday.
“This is the first oath I ever took in my life. I do not know what it means yet. I just promised to tell you the truth. I understand that I might be punished by God, if I did not tell the truth.
“My father and mother are in the room now. “I know Dr. Kannel. I remember back some years ago when I was sick and Dr. Kannel operated on me. I was in the courtroom this morning when my father told you about putting me on the pony. I remember that, and since then I have learned to ride. I have my own pony and am on him every day. I like to ride. I feel well. Since school started last September, I think I missed about three days.
“My pony and I have entered shows and have won some prizes. I have won some ribbons. It does not hurt me when I ride. That is my hobby. I play with other boys and girls in the neighborhood. “I am in the third grade.”
ATTEMPT AT REBUTTAL
Since sarcoma of the spleen in children is always rapidly fatal, and the disease had already reached the terminal stage when it was diagnosed and she was given the Koch Treatment, death would have taken her in a matter of weeks had not a truly curative process been instituted. Therefore, three years later, when this Testimony was given and the little girl appeared and testified in perfect health, there was no denying the cure. It was necessary then to deny the correctness of the diagnosis to defeat the defense. But this task presented difficulties, since by one very simple test, the jury could understand that the hardness and hard, nodular, nature of the great enlargement of this spleen, determined that it was a sarcoma and nothing else. Dr. Wirth gave the “opinion”, on rebuttal, that it was a septic spleen that is the enlargement was due to infection. But he had to admit that a septic spleen feels hard, but he did not seem to have much confidence in the strength of this argument, so he shifted to the claim that you can’t feel a spleen, anyway, to determine if it is hard or soft, for “fear of rupturing it as the capsule is too thin.”
Everyone knows that the doctor comes to the bedside and examines the spleen when a person is sick, and he uses pressure to do it, much more pressure, in fact, than is necessary, if the abdomen is opened and when one can get it between the fingers to palpate its hardness. Yet the spleen is never ruptured by such an examination. However, expert Testimony settled this matter. A following Government witness, Dr. Westphal, who came to testify about some X-ray plates, was asked, page 8817 of the Transcript, while he described the examination of the abdomen, “Q. —How do you palpate the spleen? A. —The same way on the other side. Q. —You apply pressure? A. —Yes, sir. Q. — Is there danger of rupturing the spleen? A. —Oh, no, not on palpation, no sir. Q. —Is it possible and proper to palpate the spleen by applying pressure to determine what it is? What would you determine by that? A. —Well, I always consider if I can feel the spleen, that it is enlarged. Q. —Is the spleen contained in a capsule? A. —Yes, sir. Q. —Any danger of rupturing that? A. —Not by palpation, you could not rupture it.”
Thus, Wirth failed to show that Dr. Kannel could not examine the spleen and palpate it to determine that it was very hard, nodular and so greatly enlarged, that it grew up into the chest to displace about two-thirds of the lung area, as well as, down into the abdomen. Since this hardness and the other characteristics determine that it was sarcoma, for no other disease of the spleen has such characteristics, the diagnosis of sarcoma of the spleen was established. Moreover, since sarcoma of the spleen is a rapidly fatal disease, and always finally fatal, its cure following the Koch Treatment is something new in medicine, that should interest all humanitarian Americans.
Affidavit
ALLEN COUNTY
SS
STATE OF INDIANA
“ON THE FOURTEENTH day of May 1948, appeared before me, Dr. J. W. Kannel of 1405 Vermont Avenue, Fort Wayne, Indiana, who deposeth and says, that he has practiced medicine and surgery in Fort Wayne, Indiana, since the year 1899, after practicing three years in Ohio. Ever since the commencement of practice, he had free access to the hospital facilities in Fort Wayne, and made surgery a major part of his work, and was a member of the surgical staff of the Bueyrus Hospital from 1914 until 1917, and visiting surgeon to St. Joseph’s Hospital, the Lutheran Hospital, the Methodist Hospital, and Medical Center Hospital, as a desired and honored patron.
“Affiant also says that he was a member of the American Medical Association, the Indiana State and the County Medical Societies until the year 1945, when he was notified that he was no longer a member of said medical groups. This followed charges of unethical conduct without any basis in fact and without the right of affiant to defend himself with proofs of the correctness of his methods. Affiant was charged with claiming to help cancer when the method he used was condemned by the society members, none of whom knew the first thing about the method by experience, or scientific training, qualifying them to possess an opinion. The method used by affiant was the Koch Treatment, which he found so much more efficient than surgery, which he had previously employed, but he could no longer use surgery in cancer conscientiously, but was compelled by conscience to use the Koch Treatment instead. It was for offering this method to his patients that the medical society took away his membership in these medical groups, and deprived him of the rights that pertain thereto. Affiant also states that the fact that he used the Koch Treatment was the basis of said attack upon him, although an attempt was made to assign the charges to his method of answering inquirers, as to the treatment he used. That there can be no fault to affiant’s method of reply, a form of reply was used, which is herewith given, and the usual type of inquiry is herewith also copied.
“INQUIRY— ‘I am told by a friend that you have a guaranteed cure for cancer. I am deeply interested in receiving full information for a friend of mine who is afflicted. Will you kindly forward me full particulars and especially tell me if you can assure a cure?’
“REPLY— ‘Some people recover when given the Koch Treatment, which I use. You may have a physician near you who is using it. I do not take any case unless I can first examine it. No reputable physician guarantees a cure of any disease he treats. The cost is reasonable.’
“Respectfully,
“J. W. Kannel, M.D.”
Many such inquiries were received and answers were given according to the form and meaning stated above.
“Affiant further states that on August 4, 1942, he received a letter from the Superintendent of the Medical Center Hospital of Fort Wayne, Indiana, requesting him to discontinue the use of that hospital. (This letter is reproduced as Plate 22.)
“Affiant also says that in April, 1946, he was notified verbally by the Rev. H. W. Mohler, Superintendent of the Methodist Hospital, that he could no longer operate or enter a patient into the Methodist Hospital on his own standing, but would have to have a sponsor who was a member of the Allen County Medical Society and of the staff of the hospital. This dismissal came after having operated and enjoyed the facilities of said hospital from 1925 to that date in April 1946. Affiant states that previously he had operated in all the hospitals up to 1925 after which time, he transferred all his surgical activities to the Methodist Hospital. No cause was given other than that affiant was no longer a member of the local and state medical societies and of the American Medical Association. However, affiant did then, and still does belong, to the time-honored and respected National Eclectic Medical Association, and the American Institute of Homeopathy.
“Affiant further says that he was discharged from the medical societies for “unethical conduct in the practice of medicine,” which was supposed to be an instance of an answer to a letter of inquiry, such as is noted above. No proofs were given to sustain the charges and no opportunity to demonstrate the superiority of the Koch Treatment in the care of cancer cases, as proved by results obtained in recurrent, far advanced cancer of the stomach with full obstruction, and massive involvement and terminal cachexia with full recovery permanent over twenty years, in inoperable cancer of the uterus, breast, and other parts of the body… cases that had no hope, otherwise, but were restored to health and full freedom from the disease.
“Only “opinion” by men who knew nothing about the method was raised against the affiant. Facts were not permitted in the defense.
“(Signed) J. W. Kannel, M.D.”
Subscribed and sworn to before me the 14th day of May 1948.
(Signed) Mildred Vera Verweire
My commission expires April 20, 1950.
PLATE 22. This is a reproduction of a letter sent to Dr. J. W. Kannel whose Testimony, in the Beverly Graves Case, verified the fact that the Koch Treatment brought recovery from cancer of the spleen.

Lymphosarcoma
THE CASE OF LOLA MILLER
Introductory Remarks
This is presented as a case of the type of lymphosarcoma, which grows large and kills before it has metastasized widely. It belongs to the type Ewing describes on page 422 “The more rapid cases are fatal while the growth is chiefly local.”
This patient, age thirty-one, had developed an orange size tumor in the right breast, which extended into the axilla. Cachexia was developing rapidly. On July 1, 1925, the part that involved the breast proper was removed, leaving the rest of the breast tissue and the surrounding cancerous invasions including that, which developed, into the axilla. A dose of Glyoxylide was given by Dr. Kannel on July 16, 1925. Dr. Kannel was the surgeon who performed the operation. He testified that ‘he did not remove all of the cancerous tissue and explained the reason for not doing a complete and radical operation in that his experience was that such operation would not prolong life one bit but would hopelessly cripple a patient and increase their suffering.’
This is in keeping with Ewing’s statement on page 598. “There can be no doubt that operation shortens life and aggravates the terminal sufferings in the great majority of recurrent cases.” In other words, where the skilled surgeon can see that successful operation is impossible it is useless to attempt a radical operation.
The removal of the breast lump was done to establish the diagnosis as to the type of cancer so as to be able to make an accurate prognosis. The diagnosis given herewith is a Photostat of one of the sheets of the hospital record. (Plate 23)
PLATE 23. Photostat of the Methodist Hospital laboratory record in the Case of Miss Lola Miller, establishing by biopsy the diagnosis of “malignant lymphosarcoma.”
Following the Glyoxylide, there was rapid absorption of the axillary and other cancerous extensions and a quick recovery from the cachexia.
She remained well until 1931, when a lump appeared in the left breast the size of one’s thumb. It was removed by Dr. Kannel, and was diagnosed lymphosarcoma from its clinical features only, plus the history of the former disease. Another dose of Glyoxylide was given and no further recurrences took place. Her health remained perfect. On examination in April 1946, she was found to be perfectly well.
AN ANALYSIS OF THE REBUTTAL OF THE LOLA MILLER CASE ATTEMPTED
BY DR. WIRTH
The rebuttal of this case was given by Dr. Wirth, who adapted his Testimony to the length of time she stayed cured, about twenty-two years, till now. He testified, “In my “opinion” the entire course of the disease is the result first, of the local removal of the disease, secondly, on the chronic nature of the disease, lymphosarcoma.”
Both “opinions” are contradicted by the facts in the case, for the whole disease was not removed in the first place, and in the second place, lymphosarcoma is a rapidly fatal disease. Thus, the experience of many years is summed up in Ewing’s statement page, 423 “The usual course is progressive and fatal within a few months. Wide extensions are observed chiefly with more prolonged course. After local treatment, extirpation, internal use of arsenic or application of X-ray, the disease has often appeared to be arrested only to recur after a brief period.”
It is also known that cachexia appears, in this disease, just before death. As Ewing states on page, 423 “But anemia and cachexia may not appear until toward the end of the disease.” Ewing also states on page, 422. “The more rapid cases are fatal in which the growth is chiefly local,” and “that it is one of the most malignant of diseases, resisting attempts at extirpation and proving a veritable ‘noli me tangere'” (‘Touch me not’).
Since disturbing lymphosarcoma for biopsy leads to its increased activity, and the Testimony shows there was plenty of cancer tissue left to bring about an early mortality, which was already imminent, as shown by the cachexia, her recovery could only have been brought about by a most effective removal of the cause. The only Treatment given was the Koch Treatment. It is therefore evident that the facts, in the case, were not successfully rebutted by Dr. Wirth.
Lymphocytic Cell Type of Lymphosarcoma
THE CASE OF MRS. GEORGE GROVE
Introductory Remarks
Here is another case of the rapidly developing, early fatal type of lymphosarcoma. Such cases have to be treated shortly after the disease is recognized, or they will not live long enough to be treated at all. The case under consideration now, is a fair example of the increase of the malignancy by surgical interference.
It also exemplifies the great speed with which the reverse process, the recovery, takes place. Indeed recovery is as rapid or perhaps more rapid than the disease progresses, even at its best.
Mrs. George Grove, age 40, developed a glandular swelling in the back of the right side of the neck. A mass the size of a cherry was removed on April 27, 1937. (Plate 24) Though the growth removed was only the size of a cherry, it did not stay away. Within three weeks, it had recurred at the same place as a growth at least five times as large as when removed. When she appeared at the Koch Clinic on May 17, 1937, it had become as large as half of an egg, bulging outward.
PLATE 24. A copy of the surgical pathology report of the diagnosis laboratories of the Miami Valley Hospital, in the Case of Mrs. George Grove, indicating “lymphosarcoma.”
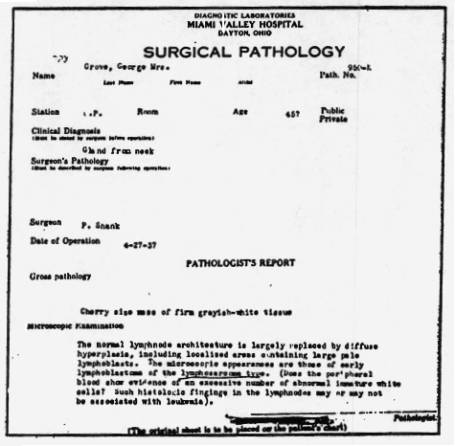
It had infiltrated deeply into the tissues of the neck and was well fixed. A few other much smaller glands were also present in the vicinity. They were the size of peas, approximately. She received her one dose of Glyoxylide on the same day, and on examination three weeks later no trace of the growth could be found. It had absorbed completely, not even leaving a scar. The several smaller glands also disappeared in this same period and her health became normal.
The history further shows that the growth first made a noticeable start about five weeks before the biopsy was done. Thus, before cutting into it the rate of growth was about one-tenth what it was after it was cut. So, the recovery process had a speed equal to the growth development at its best.
Mrs. Grove never had a recurrence after the one Glyoxylide injection and remained in good health. However, four years later she was hit by an automobile and killed. An autopsy was made but no cancer could be found anywhere in the system. Thus, this case, through the unfortunate accident, which called for an autopsy, is exceptionally valuable in showing that the disease was entirely overcome.
ATTEMPT AT REBUTTAL
The rebuttal, in this case, was given by Dr. Shank who also did the biopsy. He gave the “opinion” that he thought he removed the whole growth when making this biopsy. However, the rapid recurrence showed that he did not remove the whole growth; but simply stimulated it, in accordance with the consensus of experience and knowledge regarding this disease. It is well known that this disease does not yield to surgery, or other destructive methods. Ewing’s statement on page, 422 of his text explains this fact most concisely. ”Yet it is one of the most malignant of diseases, resisting attempts at extirpation, and proving a veritable ‘NOLI ME TANGERE’ which means ‘touch me not'” Here he also states that after extirpation it recurs “after a brief period.”
Endothelial Sarcoma of the Bone
THE CASE OF HAROLD BARNARD
Introductory Remarks
This case is best appreciated by studying the data in the hospital record, but as an introduction, a brief general statement is given first.
This patient, Harold Barnard, was perfectly healthy until forty-one years of age when he noticed pain in the right arm, with limitation of motion. Radiographs were made at his home in Jackson, Michigan. One is presented here. (Plate 25)
PLATE 25. This is an X-ray of Harold Barnard dated August 31, 1934, showing destructive Sarcoma of the shoulder joint and bones.
Then he entered the University of Michigan Hospital for complete diagnosis. The hospital record shows that several alternative diagnoses, suggested by the X-ray, had to be ruled out by blood and urine chemistry and by biopsy. It was thus established that the disease was a sarcoma of the bone arising in vascular endothelium. Since the lesions were so extensive, as to involve the humerus and scapula, and the microscopic findings showed these lesions to be a malignant form of sarcoma, the case was considered inoperable. However, the suggestion was offered that the arm and the whole shoulder girdle might be removed. He refused this operation and was given the Koch Treatment on September 17, 1934.
He was in fair nutrition, but there was a lemonish tint to the skin and eyes often found in malignant disease. He was suffering considerable pain in the right arm and shoulder. In fact, the arm had to be protected from motion or sudden jarring. He was not able to use it. Over the right shoulder blade, there was a protruding tumor mass about the size of one’s fist or a little smaller. Another lump the size of a walnut was present closer to the spine. The skin over the large tumor showed the scar of the incision where a biopsy was made and it was evident that the tumor had grown some since this was done, only a few weeks previously.
It is observed, in examining the hospital records, that the removal of tissue for microscopic examination, both from the muscle that was invaded by the cancer, and from the bone were quite bloody affairs. The malignant cells had a fine chance during all this manipulation to be spread by the blood stream to all parts of the body. Biopsies on sarcoma cannot avoid spread of the disease and where the malignant tissues are torn apart and cut as much as was done in this case, this procedure must certainly have thrown millions of malignant cells into the blood stream. Sarcoma can increase its grade of malignancy very suddenly after being scratched or pinched and the extensive rough handling that was necessary to the performance of the biopsy, no doubt, had this very effect.
As Ewing* states, page, 73, “There can be little doubt that the rough handling of cellular tumors, in the preparation of the patient and in the excision of the growth widens the field of infection by forcing cells through the vessels and tissue spaces.”
“The practice of removing a portion of the tumor for diagnosis may add to the dangers of local dissemination. Arising from the remnants of the original growth, recurrence is usually prompt, multiple in the line of incision or nearby and of the same type as the original growth, or more malignant. Local recurrences usually show increasing malignancy and anaplasia.”
It is an important observation, therefore, that this case of sarcoma did not form metastases and go ahead and die after the Glyoxylide Treatment. The malignant tissue disappeared, and instead, he recovered. Sarcoma of this type is always fatal as Ewing states, page, 361, “Angioendothelioma, multiple endothelioma, diffuse endothelioma, or endothelial myeloma, the entire group, is characterized by a predilection for the bone shaft, a tendency to multiplicity, a cellular and vascular structure, marked osteolytic properties, failure to produce tumor bone, and a relatively slow BUT FATAL COURSE.”
We can reach no other conclusion but that the basis for malignancy, the cause of metastatic activity, and malignant reproduction of cells, was removed after this Treatment. This is in contrast to the accepted type of treatment, which is to try to cut out or destroy the malignant cells themselves. This Treatment was administered at some distance from the cancer involvement, and had to act through the blood stream on every cancer cell.
The first radiograph taken before Treatment in August 1934, demonstrates the characteristics just mentioned by Ewing for sarcomas originating in the lining cells of the blood vessels. The destruction of bone substance demonstrated in these pictures is discussed in the University of Michigan Hospital report, as a process to be differentiated from that in Paget’s disease of the bone, myeloblastoma, and where the bone is attacked by benign and malignant giant cell tumors, for these had to be excluded in arriving at the exact diagnosis.
(* Ewing is universally recognized as the greatest authority on the clinical and microscopic features of cancer.)
To do this, the conclusive test, the biopsy, was made though it did endanger spread of the disease. The biopsy proved the growth to be a malignant cancer. The blood analysis reported here rules out Paget’s disease. Thus, the diagnosis is established beyond any possibility of doubt. The recovery is also established, since instead of dying in from a few months to a year, or so, he got well and is still well fifteen years after Treatment.
The second X-ray shows the healed bone. This was taken in 1942 during Dr. Koch’s first trial. This shows that instead of being subjected to a destructive process, the bone was restored by the production of a thicker shaft wall and many small trabeculae or bone septa, which restore the structure of the spongy part of the bone.
His arm is able to function normally again. It is as good as it ever was and as good as the other arm that always was well. The malignant growths have disappeared leaving in their places stronger and thicker bone only. Thus a good restoration to normal has taken place. (Plate 26)
PLATE 26. This is an X-ray of Harold Barnard taken in 1942 at the time of the Koch Hearings, showing recovery from the malignant sarcoma of the shoulder joint and bones.
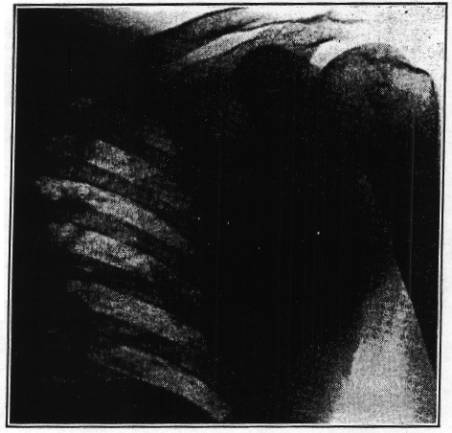
Mr. Barnard’s account of his experience is given herewith.
TESTIMONY OF HAROLD BARNARD
“Back in 1933, I started having trouble with my arm, the right upper arm. I thought it was neuritis or something of that nature. There was pain there. It was intermittent, usually worse at night when I went to sleep. I noticed a small lump on my right shoulder blade. It became worse as time went on. At first it did not interfere with my ordinary work, and then I threw a ball at a picnic and in throwing the ball, I must have done something to the arm.
“From then on it was practically useless. I could not write or shift gears on the car.
“I went to see a Dr. Brown and he sent me to the University of Michigan Hospital. That was during the summer of 1934. They took some X-rays and a biopsy.
“In the middle of September, 1934, I went to Dr. Koch. He gave me an injection. I had reactions in the form of the grippe. It was a matter of weeks before I noticed my arm changing. It was a year or two before I felt that I had recovered the complete use of the arm, as I was favoring it, naturally. Now I do not favor it at all, I can use it in any endeavor I wish to use it. The lump on the back has practically disappeared.
“The scar on the back starts 2½ inches to the left of the right armpit and goes down in a diagonal direction about a distance of three inches or three and one-half inches.”
THE ATTEMPT AT REBUTTAL
The rebuttal in this case was offered by the “opinion” Testimony of Dr. Birkelo, who thought it might be a benign, giant cell tumor, and by Dr. Wirth, who thought it might be a case of osteitis fibrosa cystica. Both of these “opinions” were based upon X-ray pictures and were also considered by the experts at the University of Michigan Hospital to whom the X-rays, in addition, suggested the possibility that the disease might be a multiple myeloma.
The “opinions” of the rebuttal witnesses do not agree with each other. But, the three possibilities mentioned were set forth and considered by the University of Michigan Hospital staff on the basis of the X-ray findings. The incorrect “opinions” offered by Dr. Birkelo and by Dr. Wirth were ruled out, both by making a biopsy, and by studying the blood chemistry. (Plate 27)
PLATE 27. A copy of the University of Michigan pathological specimen report, in the Harold Barnard Case. Note that it describes his condition as “a malignant neoplasm.”
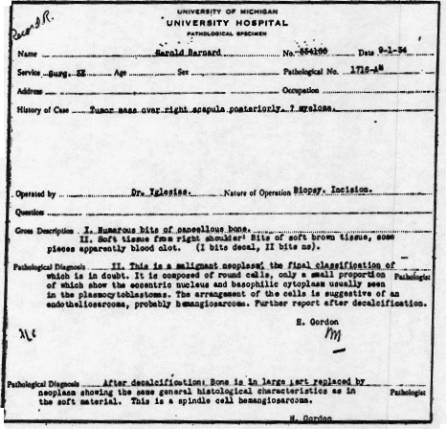
The biopsy revealed a specific type of sarcoma, which is very definite in its structure and which could not possibly be confused with osteitis fibrosa cystica, or with giant cell tumor, or even with multiple myeloma. It was found to be a malignant growth, without the least doubt and of the type called endothelial sarcoma. Microscopic studies of osteitis fibrosa cystica show that this disease is not a tumor at all, but a loss of calcium from the bone structure, plus reparative fibrosis. The microscopic picture of giant cell tumor shows that it is made up of cells, each of which is about one hundred times as large as and contains sixty to one hundred times as many nuclei as the small simple cells, which make up an endothelia sarcoma. These small cells contain only one nucleus each. Hence there could be no possibility of confusion for the pathologist who examined the specimens.
“On cross-examination, Dr. Wirth claimed he could not tell the difference between the giant cell of a giant cell tumor and the spindle cell of an endothelial sarcoma, which as we have just indicated, are as different from each other as an autobus and a wheelbarrow.” Moreover, the blood and urine chemistry (pages 55, 56, of hospital record) supported the biopsy showing that neither osteitis fibrosa cystica nor a benign tumor was present. No fact witness was produced to show error in the interpretation or description of the biopsy specimens; both of which checked perfectly and also agreed with the gross characteristics of the tumor where it broke through the bone and invaded the soft tissues outside the bone, forming a very vascular growth with marked hemorrhagic nature, as described by Ewing on pages, 361 and 366.
He also shows here that fibrosa osteitis cystica exists simultaneously with endothelial sarcoma and that although some cases only live a few months, some may live as long as two or three years, but that the disease is always fatal. The recovery of this patient may be considered a cure, since he remains well now about fifteen years, instead of the upper limit of three years, which in this form of progressing disease ends in death. If there was any fibrosis osteitis present to complicate the disease, this hitherto “incurable” disease was also cured. So in this case, a most marvelous curative ability is demonstrated in the body following the Glyoxylide injection.
Dr. Birkelo gave the “opinion” that the disease was cured, or might have been, by a bump on the elbow, which the patient might have sustained. Thus, a disease so serious in the opinion of the University experts that even removal of the arm and shoulder girdle would fail, could be cured by just bumping the elbow, in the “opinion” of Birkelo. Here we see how competing surgeons become panicky when confronted by the successful Treatment of a cancer case.
A study of the recovery reactions shows that the cyclic features that are uniquely characteristic of the Koch Treatment identify the cure as belonging to this Treatment and it alone. The facts, thus, contradict the “opinions” of the Food and Drug Administration “experts.”
Quotations from Ewing which confirm the factual features of this case follow:
“While intermediate types of tumors occur, three structural varieties may, for the present, be recognized: (1) Angioendothelioma. (2) Multiple endothelioma. (3) Diffuse endothelioma or endothelial myeloma. The entire group is characterized by a predilection for the bone shaft, a tendency to multiplicity, a cellular and vascular structure, marked osteolytic properties, failure to produce tumor bone, and a relatively slow but fatal course.” (page, 361)
“The growth is rather slow, occupying several months; it is accompanied by pain and disability and often results in spontaneous fracture, which may be the first prominent symptom.” (page, 361)
“Osteitis fibrosa is sometimes seen in the unaffected bones, and may be detected in the roentgenogram.
”The total duration of the disease varies with the histological malignancy, and with other factors. Some subjects succumb to very rapid growth of the original tumor, and widespread secondary tumors in a few months, while others survive for two or three years. The course is, therefore, much slower than with osteogenic sarcoma.
“The mortality is very high, especially with the younger subjects.
“GROSS ANATOMY. —In the earliest stages, a considerable area of bone marrow is found to be cellular, and opaque from focal and diffuse proliferation of tumor cells. This process spreads through a large portion of the shaft, and displaces the weakened shaft outward. New bone may be laid down by the periosteum in very characteristic parallel lines or irregular deposits, but the periosteum is soon perforated, and the tumor tissue infiltrates and displaces the soft tissues, forming a fusiform, soft swelling. Most of the tumors are very vascular, and subject to rapid fluctuations in volume. Hemorrhage and necrosis occur in the central portions.” (page, 366)
The gross pathology described in the operative record fits this description by Ewing perfectly and so the diagnosis is again established and the rebuttal witnesses put to shame.
Far Advanced Cancer of the Colon In The Terminal Stage
THE CASE OF JOHN KELLY
Introductory Remarks
In this case, the patient had been ailing with a painful abdominal complaint giving various diagnosis, such as diverticulitis, etc., until obstruction of the bowel took place near the splenic flexure, and a rapidly developing cancer formed an enormous tumor that spread through the abdomen and ruptured through the abdominal wall on the left side. A fistula was thus formed that permitted the fecal material to empty out over the abdominal wall. This fistula enlarged rapidly, as the malignancy advanced to form a large cauliflower growth upon the surface. Several other fistulae formed in the same way emptying feces over the abdominal wall. Biopsy was performed and the true nature of disease was thus proved to be a very malignant form of cancer of the colon. Exploration proved the disease to be so far advanced and to have spread throughout the abdomen and to have invaded the wall so widely that it was entirely hopeless and inoperable. X-rays showing the obstruction, was made at the Henry Ford Hospital, are described in the hospital record extracts in the publisher’s file. The description of the exploratory operation and the hopeless condition is likewise given. One radiograph made early in the diagnostic observation period is reproduced here.
After the exploration the patient’s condition degraded rapidly, as would be expected in a case of such virulent malignancy. He lost much weight, became very weak, and was given an early terminal prognosis as the hospital record shows. (Plate 28)
PLATE 28. This is a copy of the general memo from the Henry Ford Hospital regarding the Case John Kelly. Note that the diagnosis indicates a “fungating carcinoma of colon.” Especially note the remark at the bottom of the memo: “This is entirely a hopeless case.”
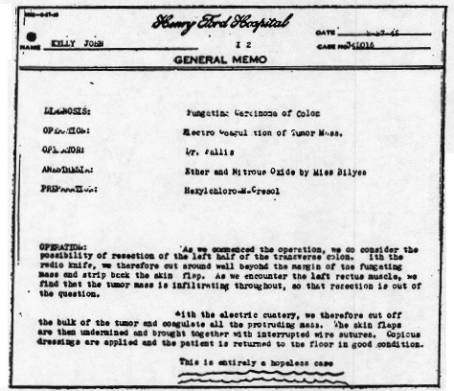
He was then given the Koch Treatment and was a little better for a while, but at the fourth week following the injection he showed evidence of too much exhaustion to react profitably, so he was given another Treatment. Recovery came rapidly after this, and as the record shows, he gained in weight and strength very rapidly, like some other badly emaciated cases have done, following the Koch Treatment. He went back to work in a couple of months. As he recovered in this period, the growths that had perforated the belly were absorbed, and the destroyed areas healed beautifully.
The invasion of the intestines and abdominal structures by the malignant tissue also underwent involutions and absorption. In this way, the obstruction was also cleared away and the intestinal wall healed so it could do its work again. In fact, within six months after the Treatment, the obstruction of the bowel disappeared and his colostomy was not needed anymore; and although some fecal matter leaked through, the majority of the bowel movement came through the rectum again, in a normal way. Dr. Koch then advised that the opening in the colon (colostomy) be closed. This was done on November 23rd, 1942, as is recorded in the hospital record.
THE TESTIMONY OF DR. F. L. RICHARDS
“I first saw John Kelly in March, 1942 at our nursing home. He was removed from the Ford Hospital to the nursing home and stayed there one day. His wife came to the office and told me about the case.
“When I saw him he had at least three openings in his abdomen. They were all discharging fecal matter, and the skin was denuded, more or less, from the toxic condition, and what was considered cancerous tissue was pressing out of the abdomen, in at least two of these openings to the extent of perhaps one inch. It must have been cancer in my opinion. I don’t know what other disease would take that form. There was something peculiar about this tissue, the nature of it, and the history of the case. He had been operated on for a growth in the bowel, and the incision had broken down and this condition had developed following that condition.
“There was a lot of odor from that fecal matter, that was why we couldn’t keep him at the nursing home, but one night. The odor was so terrible that we had to move him from there.
“I gave him an injection of Glyoxylide, and they took him to his home near Ypsilanti. I saw him once a week from that time on, until the latter part of May, and then I was out of town for three weeks. When I came back, I found him very much improved. He had gained some twenty pounds in that three weeks, and was looking and feeling fine. I examined the abdomen and it looked very normal, the growth had all disappeared. He was sitting up in a chair and said: ‘I don’t need you any more. I am getting along fine.’
“After the first visit, I made several visits there a week apart, and his condition remained about the same. At the beginning of the fourth week, after he had received the first Treatment, I gave him another Treatment because he didn’t seem to be improving, as I thought he might. He had been subject to hemorrhages from the bowel at that time, and I also gave him some calcarea for the bleeding. The fourth week, I gave him the second Treatment, and he seemed to improve from that time on.
“In my opinion, the disease was cancer from which he was suffering. I saw him once or twice after the 15th of June. Now he is working every day at the Bomber Plant.
“He was on the Koch Diet, as long as I was in attendance on the case, and when he went to the Ford Hospital for later treatment, his wife told me that they kept him on the same diet when he was in the hospital.”
THE TESTIMONY OF MRS. ALTA KELLY
“I am John Kelly’s wife. The first time he went to the hospital in 1941, he complained of not feeling good, and he would be tired. The night we took him to the hospital he didn’t sleep all night. He broke out with sweat, and rolled and tumbled, and was unable to get up the next morning. He came home from the hospital after an operation, and went back to work in November 1941. December 17th, he stopped working. He went back to the hospital for three or five days for observation, right after Christmas. They took X-rays. (Plate 29)
PLATE 29. This is an X-ray of John Kelly taken by Henry Ford Hospital showing the condition of his colon. Exactly two months after this X-ray was made, this case was judged to be entirely hopeless by the hospital.
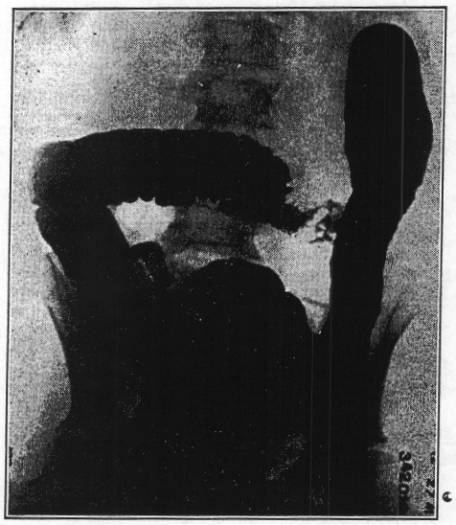
“He grew gradually worse all through the month of January, the last week he was in bed. The first day of February, he was taken back to the hospital in an ambulance, and they performed a colostomy. As far as the colostomy was concerned, it was proving satisfactory, but his stomach still continued getting worse, and he had these pains. The incision was opening up, and there was a discharge, so they dressed it. There was an opening in the abdomen from the first operation that they had never thoroughly closed, and there was drainage.
“On February 27th they operated again. He got out of the hospital April 1st. The opening was still there, still getting larger and discharging very much fecal matter. This opening was across the abdomen where they had cut him open the first time. The colostomy was one opening, and where he had been operated on there were two openings. Beside where they had sewed him together with wire to hold the incision together, there were three or four others that would open up, and they were gradually getting larger. On the outside of the large flesh, and as each one of these places opened up, there was a growth that would come up out of these. It looked rather like raw beef, and had an awful odor.
“About the middle part of April, he got so he could get up and go outside. Then he had a hemorrhage. It started on a Sunday, and the following Saturday he hemorrhaged from two to four, and from ten to eleven that night. The hemorrhage came from the wound in his stomach. It seemed to come from the inside of his stomach. Dr. Richards came out and gave him another injection, and gave him some medicine to clot the blood and stop the hemorrhage.
“The liquid that came from the wound would seem to irritate the flesh, and make it very sore. He was very low at that time. He could hardly raise his head off the pillow. He didn’t want to eat. Three or four weeks after he had the second injection, he was taken with a terrible chill. Apparently after he got over that he began to get better. He got up the latter part of June of that year and went back to work. The colostomy is closed, working very good.”
TESTIMONY OF JOHN KELLY
“I had very much pain in my abdomen off and on for about six months. I went into the Ford Hospital in 1941, and was there forty-one days. They operated on me after nine days. I went back to the hospital in January 1942, and was very ill when I came out. I had a colostomy operation. Dr. Richards gave me a shot some time in April, and another one about a month later.
“I went back to work in August. I went to the hospital in September, and they put a clamp on my colostomy, and again in November, I went to the hospital. That was to finish closing it. After the second injection I improved a lot. In the latter part of June 1942, I weighed 113 pounds, and I must have weighed less than that, because this was when I was able to get out of bed. Now I weigh 184½ pounds.”
AN ANALYSIS OF THE REBUTTAL IN THE JOHN KELLY CASE ATTEMPTED BY DR. WIRTH
The rebuttal offered was Dr. Wirth’s “opinion” that the recovery resulted from the surgical activities and from the infection that was present. This, as one may see, on page 12 of the hospital record, date 2-27-42, is untenable, since the results of the exploration are recorded. ‘This is entirely a hopeless case.’ It is moreover, well known, that when cancer becomes infected it also becomes more rapidly fatal and progressive. Ewing states this on page 17 of his text. The quotation will be given shortly with others.
To further show that the Wirth “opinion” has no basis in fact and is contrary to established knowledge regarding cancer, we point out that the exploratory surgery only went the depth of the abdominal wall when it encountered so dense an invasion of cancer that the exploration had to be stopped before the abdomen could be entered and explored. The place of origin of the growth could not even be approached. The biopsy was taken, therefore, from the extension of the cancer into and through the abdominal wall and is so indicated in the record as, “Metastatic Carcinoma.” However, the fungating mass that ate through the abdominal wall caused so much odorous discharge that it was sliced off and the surface cauterized to stop bleeding. However, Dr. Wirth hazards the “opinion” that this superficial trimming and cautery removed the whole cancer, with the help of the infection that caused so much bad odor.
The facts show that the great involvement with cancer throughout the abdomen was not even touched by the surgeon so they recorded, “This is entirely a hopeless case.” Only the surface was trimmed. Established knowledge set forth by the authorities shows that instead of helping, the surgical procedures could only stimulate the growth to greater destructive activity. The further history of this case proves that this is exactly what happened. Thus, Ewing states on page 73, “There can be little doubt that the rough manipulation of cellular tumors in the preparation of the patient and in the exclusion of the growth widens the field of infection by forcing cells through the vessels and tissue spaces.” Also, “Arising from remnants of the original growth, recurrence is usually prompt, multiple, in the line of incision or nearby, and of the same type as the original growth or more malignant.”
On page 44, Ewing also states, “Rapid and progressive multiplication of tumor cells without notable intermission or hindrance, is characteristic of highly malignant neoplasms.” On page 17, “The onset of ulceration, frequently transforms a comparatively harmless tumor into a rapidly fatal process, through local or general infection, suppuration, absorption of toxic products and hemorrhage, to which chiefly must be attributed the cachexia.”
On page 597 and 598, “Statistics favor the conclusion that operation on the whole shortens life in recurrent cases.” Thus, it is evident from the established knowledge as well as from the events taking place in the Kelly Case, before receiving the Koch Treatment, that the surgery and infection could only make the disease worse and could not and did not cure him at all.
To rebut the recovery in this case, factual proofs regarding the state of the patient at the time the rebuttal was going on in court, should have been given. No such fact Testimony was produced, even though Mr. Kelly went from Montana to Detroit, so that the Ford Hospital experts could thoroughly examine his abdomen to ascertain if cancer were still present. The results of this examination were available at the time the rebuttal was going on, but no witnesses were produced by the Government to tell what the examination revealed. Why did the Government keep the facts secret? If the patient still had cancer, they surely would have made a report before the jury. Their silence, in view of the fact that he was studied for rebuttal purposes, is certainly significant. Anyway, he is in perfect health and has been running a large farm doing more than an ordinary man’s work. There is no symptom or sign left of his former disease. It might be pertinent to mention an occurrence outside of the Court Testimony, namely that Surgeon General Ernesto De Oliviera, of the Brazilian Army, just retired, was visiting America at this time, the summer of 1946. While being entertained at the Henry Ford Hospital, he was told by the surgeons that this case was examined recently by them and found cured, a case that they were unable to help.
Terminal, Far Advanced Case of Cancer of the Liver
THE CASE OF MARY GORDON
Introductory Remarks
There is no argument about the fact that all tumors originating in the liver are fatal. This is especially true when large portions of the liver are involved, and when the condition has progressed to a point where the patient is in a coma, and jaundice is deepening in spite of well established gall bladder drainage to the outside.
There are roughly two classifications of primary cancer of the liver. One type is characterized by a few large masses of cancer; the other type presents many small tumors that permeate large portions of the organ, and can be seen to cover one or more surfaces. These tiny pea size growths develop within the lobule from the parenchyma and cause obstruction of the minute bile ducts within the substance of the liver. They thus cause a jaundice that increases as the disease advances, even while the large bile ducts are clear.
Various names have been given to this form of cancer of the liver by the various observers who have described it. It is a type of adenocarcinoma with more or less attendant, scant or dense cirrhosis. All are agreed, however, that the condition is fatal, and a rather rapidly growing, quickly fatal, type which causes death fairly soon after the jaundice is well established.
The Case of Mrs. Mary Gordon, which Dr. Arnott describes here, is one of the latter types, a terminal case of fatal cancer of the liver. So well known is the fatality of this type of liver tumor that a biopsy is not needed and indeed one can accurately describe the microscopic picture from the gross finding. They agree with Ewing’s description of cancer of the liver on page 746, and with Cecil’s on page 862.
Ewing states, “No sharp division exists between multiple adenoma without cirrhosis, multiple adenoma with cirrhosis, and carcinoma. Each of these conditions exhibits progressive, invasive, and malignant tendencies (Muir). With the onset of the tumor process there are added increasing anemia, cachexia, diarrhea, and hemorrhages, and the disease progresses steadily to a fatal issue. After the appearance of ascites, the duration is seldom more than a few months and often only a few weeks.”
“The surface presents multiple, projecting, yellowish, or bile-stained nodules, which on section may be found to represent a large part of the parenchyma. The nodules may be numerous, small, and almost confluent, or larger, discrete, and encapsulated. One portion of the organ may be quite free, but frequently the lesion is nearly universal.”
“Many authors describe a diffuse form of hepatic carcinoma (Eggel, Rolleston). Yet these cases commonly represent a very extensive development of nodular carcinoma in a cirrhotic liver, and not a diffuse growth of tumor cell.”
Cecil states, “DIAGNOSIS, —An insidious onset with progressive nodular enlargement of the liver, anemia, and loss of weight and strength in a person at or past middle age are characteristic signs. The diagnosis is conclusive, if a primary malignant growth elsewhere be demonstrable. The presence of jaundice and ascites is additional evidence. Aspiration biopsy is a justifiable procedure in doubtful cases.”
Here is an unmolested case, one that can be estimated fully from surgical findings and terminal clinical stage where the pathology was promptly reversed, after instituting the Koch Treatment, as this attempts to establish the catalysis of oxidation belonging to the chemistry of the Carbonyl group, carried by chemical compounds of certain specific structure. The recovery was prompt and complete, and has so remained to this day, seventeen years. How many thousands of such cases have suffered and died without even hearing of the Koch Treatment in these seventeen years? What should be the objection to offering a harmless Treatment, that has enjoyed this success, to a hopeless victim of cancer of the liver?
THE TESTIMONY OF DR. DAVID ARNOTT
(Note: The following is paraphrased from the Testimony of Dr. David Arnott, in the Mary Gordon Case, as found in the Official Court Record at the Koch Trial. The words below are those of Dr. Arnott.)
“Dr. Ernest Williams, the surgeon that performed the operation on Mrs. Mary Gordon, first consulted me in her behalf. He is also of London, Ontario. Mr. Gordon, the husband of the patient, also called upon me in behalf of his wife.
“From the hospital records and speaking with the surgeon, it was evident that an operation was performed upon Mrs. Gordon on June 29th, 1931, in which the surgeon opened the abdominal wall over the gall bladder area. The gall bladder was brought up to the surface of the incision by forceps and held there while a tube was inserted to drain off the blood, and then the gallstones were found and removed. Then a permanent drainage for treatment was left there after the operation, and it was still in position when I saw her over three weeks later.
“At the operation an examination was made and no gallstones were found to obstruct the flow of bile into the bowel. It was found, at this time, that there were tumors on the liver. An obstruction of the gall bladder was thought responsible for Mrs. Gordon’s yellowish looking skin. If nothing else happened, her skin would become normal as the condition was corrected. However, Mrs. Gordon’s liver had numerous tiny, firm nodules, which would obstruct the free normal functioning of the liver, so that the bile would be absorbed into the blood and would also result in the yellowing of the skin. It appears from the hospital record of July 7th that the patient is intensely jaundiced and is feeling very miserable.
“This would suggest that the liver condition was responsible for her failure to recover after the gallstones were removed. Upon this same day the hospital record says that her condition is poor and the prognosis is poor that is hope for her recovery is poor. Reports on July 13th and July 22nd, 1931, of the hospital record, indicate that the patient still feels very sick, nauseated, and that the intense jaundice persists with prognosis still poor. “On July 24th, the hospital record indicated that the patient is still very jaundiced, has no relief from gastric pain and nausea, and that prognosis is bad; in other words, no hope for recovery. It was about this time that I first visited the patient. The hospital record indicates that I injected Dr. Koch’s Glyoxylide on July 23rd. In my opinion, no X-ray treatment, radium treatment, or operation, could have cured the patient. The opinion of the hospital, itself, stands on record as no hope for recovery. She was comatose; the gravity of this serious state was increasing.
“I gave Mrs. Gordon the Glyoxylide in the morning, as I remember, and when I saw her in the afternoon her jaundice seemed distinctly relieved to me, and by the next morning anybody could see it. From July 26th until August 10th, I was out of the country. When I returned to Canada I went to see her at Victoria Hospital. Her condition was much improved. She had lots of stomach distress, but the jaundice was much relieved and her vitality was distinctly better. I saw her at the hospital and two or three visits afterwards. She was making distinct improvement. It is my opinion that Mrs. Gordon would have died within a few weeks, if she had not had the benefit of the Koch Treatment.
“Mrs. Gordon became completely well within six months following one dose of Glyoxylide, 1931, and has remained in perfect health all these years. She is still in perfect health.”
AN ANALYSIS OF THE REBUTTAL IN THE MARY GORDON CASE ATTEMPTED BY DR. COLLAR
The rebuttal in this case, is the “opinion” of Dr. Collar that the diagnosis may not have been correct and that the condition might have been due to an inflammation of the liver caused by the blocking of the flow of bile from the liver, by a stone in one of the ducts leading from the liver. The “opinion” witness did not have the opportunity to see the liver at the time of operation, nor did he see the bile flow out freely from the tube in the gall bladder for a month or so following the exploratory operation. He did not see the patient at all, and was not personally acquainted with the facts, as they existed, so he did not see by personal observation that there was no obstruction to the flow of bile from the liver for a whole month between the time of operation and the time the Koch Treatment was given.
You will see, therefore, that his “fancies” did not agree with the facts. The facts show that the operation of draining the gall bladder to the outside was successful and the bile drain was free and not obstructed; hence, any inflammation that might have been caused by bile stoppage had plenty of time to disappear and with it the jaundice, before the Koch Treatment was given. On the contrary, the jaundice deepened while the bile flow was free, and thus, must have been caused by something else, which in itself was increasing in severity. The answer to this is the large number of growths that were developing throughout the liver. It was an involvement of large areas accentuated on certain surfaces and follows the description, which Ewing gives of cancer of the liver. This characteristic of large areas involved with the small tumors, and others not involved, also eliminates Dr. Collar’s “opinion” that the condition resulted from inflammation due to obstruction of the common bile duct. For such obstruction would affect the whole liver uniformly throughout, and not only in patches, as cancer does. The rebuttal “opinions” do not apply to this case, therefore.
Cancer of the Pancreas Diagnosed by Exploratory Operation
THE CASE OF MRS. VIOLA WHITE
Paraphrase of the Testimony of Dr. Rosa Barr
“My name is Dr. Rosa Barr. I live in Cleveland Heights. I am a graduate of Cleveland Homeopathic and have a certificate from the Ohio State University. I was graduated in 1904 and commenced practice in Cleveland immediately and have been there ever since. I am on the staff of Woman’s Hospital and on the visiting staff of Huron and Fairview Hospitals. I hold a physician and surgeon’s certificate, but have not done any surgery for several years, due to the fact that my left arm and shoulder were crushed in an accident and I have little use of the left arm.
“I have been the physician of Mrs. Viola White for about thirty years. On that afternoon in September 1938, I was called by Mrs. White. I found her in intense pain. The abdomen was very rigid. It was not definitely located over the appendix; in fact the pain came in spasms. I figured it was acute appendix, but it was difficult to decide definitely. At the request of the family, I called Dr. John Hepple. He came and he felt the same as I did about it. We took her to Huron Road Hospital between seven and eight in the evening and the operation took place immediately. (Plate 30)
PLATE 30. This is a copy of the operative record made by the Huron Road Hospital surgeons in the Case of Viola White. This exploratory operation showed a “tumor at head of pancreas,” which the three physicians attending the operation, according to Dr. Barr, one of them, agreed was cancer and that the case was inoperable.
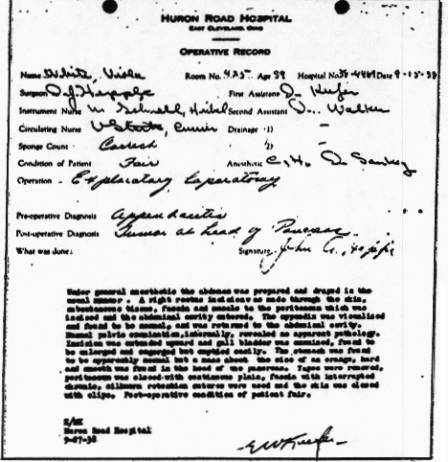
“I was present at the operation, as an adviser, but could not perform it myself because it was only a short time after the accident, which injured my left arm. After some investigation, they, Dr. Hepple and Dr. Balotti, both of whom are now in foreign service, found at the head of the pancreas a sort of mass that was about the size of an orange and it had infiltrated over to the stomach.
“The stomach was absolutely normal and Dr. Hepple just released the pancreas from the stomach and closed up. The tumor felt soft, but it was definitely nodular. I personally felt it, as well as, the other two physicians. It was just a small area of attachment to the stomach, maybe taking the area of an inch or an inch and a half. The diagnosis of all three of us was cancer of the head of the pancreas. Nothing was removed because the surgeons felt the case was inoperable.
“Dr. Hepple took care of the patient while she was in the hospital. After she was brought home, I took complete charge of her once more. Mrs. White contracted hypostatic pneumonia after the operation, but she got over that. I did not think at the time, immediately following the operation that Mrs. White would survive. It was considered a hopeless case. In fact, when her husband asked me how long she could live, I told him six months.
“I did not know anything about Dr. Koch at this time. Dr. Wingate, a practicing woman physician in Cleveland, suggested the first injection in my presence. After this shot, she seemed easier. Upon the suggestion of Dr. Wingate, I personally administered an identical shot in the arm on the 11th of November. Mrs. White received one additional injection about six months later. This was after I advised Dr. Koch of the progress of her case.
“I gave Mrs. White nothing else. Her case was an absolutely hopeless cancer case. She is now completely well and in good health. I can only conclude that it was the Koch Treatment, which helped her. I examine her at least once a year. The cancer enlargement could be felt by palpation, but inside of a year it was completely gone. It has been a number of years and Mrs. White is still in good health.”
A PARAPHBASE OF THE TESTIMONY OF MRS. WHITE
“My name is Mrs. Viola H. White and I am a housewife living in Cleveland, Ohio. My husband is the Secretary and Treasurer of the Mutual Drug Company of Cleveland. I have lived there about thirty years.
“Dr. Rosa Barr has been our family physician for thirty years. On the 15th of September 1938, I was taken with an attack of nausea at the university Y. M. C. A. where I was attending a luncheon. After I was brought home, I called Dr. Barr immediately. She came and then I was taken to the Huron Road Hospital. Before I went to the hospital, however, Dr. Barr had called in a Dr. Hepple, as a consulting physician. Dr. Hepple is in the armed forces at present. He said I should be taken to the hospital at once. That same night I was operated on and remained in the hospital for about two weeks. I was in bed about six months altogether under Dr. Barr’s care.
“I suffered a great deal in my stomach for two or three weeks. These pains continued right up to the time I had the first injection of Glyoxylide. I felt much better and gradually came to be more comfortable. I had a total of three injections between October 1938, and March 1939. I have been in perfect health since and have had no recurrence of the difficulty. I am now back to my normal weight.”
AN ANALYSIS OF THE REBUTTAL IN THE VIOLA WHITE CASE ATTEMPTED BY DR. WIRTH
Rebuttal in this pancreas case was given by Dr. Wirth, who hazarded the “opinion” that the growth was an inflammatory affair rather than cancer. Of course, an inflammatory affair the size and shape of an orange would have to be an abscess; and an abscess of the pancreas would not reach that extent, without causing high fever, great pain, and vomiting, and would have demanded a much earlier operation, special drainage, etc.
An abscess of the pancreas could be recognized by the surgeon, and it would have been opened and drained or the patient would have died. This growth was not opened and drained and the patient did not die. So, it was not an abscess.
On the contrary, the facts show that instead of having the characteristics of an inflammation, it was a nodular growth, which had infiltrated the stomach as cancer of the pancreas has the habit of doing. It had infiltrated other surrounding structures as the record shows. Dr. Wirth’s “fancies”, therefore, do not agree with the facts. This Testimony characterizes the purpose of the attack on Dr. Koch.
Cancer of the Palate, Recurrent After Operation
THE CASE OF MR. ABRAM JOHNSON
Introductory Remarks
It is so well established that unless cancer is fully and completely removed at surgical operation so that not even one trace of it remains, it will come back and generally with much increased malignancy and destructiveness, and a more rapid tendency to spread. The Case of Abram Johnson, here given, shows that even in a simple, readily accessible case of low-grade malignancy, surgery can fail and also bring about a rapid recurrence with widespread dissemination of the disease. Here again it is seen that though the disease is made inoperable, the use of an appropriate antioxidant can be followed by a recovery.
Mr. Johnson, age sixty, was first seen by Dr. Koch December 1st, 1932. His condition was cancer of the palate — the roof of the mouth, and of the glands in the neck. Examination showed the palate, hard and soft, to be covered with a large growth and about a dozen smaller ones. Some of the glands under the jaw and in the neck, close by, were enlarged, fixed and hard. He gave a history of having been at the University Hospital at Ann Arbor, Michigan, October 15th, 1931, where an operation and touching up with electric cautery was done. The areas healed and all was well for a number of months and then many growths of the same type returned and were widespread; and in addition caused considerable neck involvement.
From the history of the University Hospital a Photostat is presented to give the details of the diagnosis and of the operation. (Plate 31)
PLATE 31. This is a reproduction of the University of Michigan Hospital pathological specimen report in the Case of Abram Johnson. The final diagnosis was made as “cornifying squamous cell carcinoma arising in a papilloma” on the palate.
After the Glyoxylide was administered on December 3rd, 1932, he had a series of reactions with grippiness, chills, and fever at intervals, and there was appreciable improvement even in a week. The recovery progressed steadily so that in less than a year it was complete, all tumors had been absorbed and healing was perfect. He also gained good body weight and became stronger and enjoyed better health than he had experienced for many years and still remains well, without recurrence of the trouble, sixteen years after the Treatment.
A PARAPHRASE OF THE TESTIMONY OF ABRAM JOHNSON
“I have been a watchman at the All Metal Products Company in Wyandotte, Michigan, for practically thirteen years. I was on nights for the first three and a half years and now I am on days all the time.
”I am seventy years old. If I remember right, it was on the 12th day of August 1931, that I went to the University of Michigan Hospital in Ann Arbor. Prior to that time, I had seen a doctor in Wyandotte by the name of Dr. Nagle.
“I had a growth in the back part of my mouth, way back, and it was giving me some trouble and I did not know what it was. I did not pay much attention to it for a little while. One morning I was sitting in a chair and I dozed off to sleep. It seemed when I woke up this place in my mouth just turned outside of me. I could hardly get it out of my mouth; it was so thick. It was down in my mouth. At that time that was the only growth I had in my mouth. This incident occurred on Friday night, as I recall and I went into Dr. Nagle’s office on the Saturday morning. He did not give me any treatment at all for it. (Plate 32)
PLATE 32. Copy of a letter written by Dr. A. C. Furstenberg of the University of Michigan Hospital to Dr. John Nagle regarding the Abram Johnson Case in which he confirms that Mr. Johnson’s condition was diagnosed as “cornifying squamous cell carcinoma.”
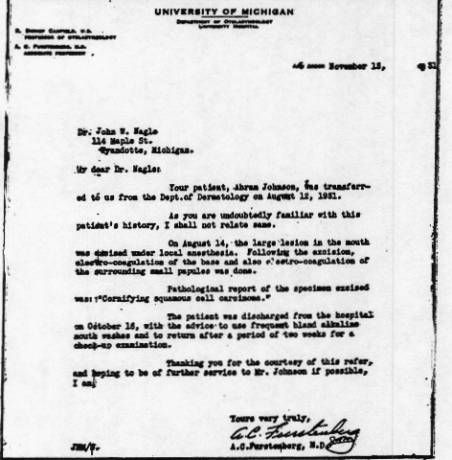
“He advised me to go to Ann Arbor at once, not to hesitate. I then went to the University of Michigan Hospital at Ann Arbor, where they examined me for about one full day. I do not remember how many doctors examined me but there were a lot of them, and also a lot of nurses that examined my mouth along with the doctors. This was on Monday and I believe the operation was performed on Thursday.
“They did not put me to sleep for the operation. I believe they injected something into my mouth. It was numb; there was no feeling.
“I went into the hospital on Monday morning and I left there on Friday evening of the same week.
“For a while my mouth was not so sore, the soreness was there, of course, but it seemed to kind of go away for a short time and then later on it began to get sore again.
“There were some small growths that came around in my mouth back where this last one was taken out. As well as I can remember now, there were nine places that came around right back where that one was and around the outside, of where it was taken out. They hurt and it was pretty hard for me to swallow and get anything back there without causing it to hurt me.
“I went back to the hospital in Ann Arbor twice before I was released from the hospital. They did not give me any treatment, just looked at me. I also went to Dr. Nagle again. He did not give me any treatment or medicine or anything of that kind. The day following my visit to Dr. Nagle, I went to see Dr. Koch and he examined my mouth. I followed his advice regarding diet and things of that kind, and in three days I went back and Dr. Koch gave me an injection in my left arm. This was in the year 1931. * About the third day I felt pretty badly. I became cold. I thought I was going to freeze. The wife put me to bed. We had the hot water bottles and about all the blankets we had to cover the bed were on me. It lasted possibly an hour. About three weeks from that time, I had another cold spell, not as bad as the first. I had those cold spells for, I would say, six months, I believe, every three weeks, but they kept getting lighter.
(* Note: There is a date error in Mr. Johnson’s Testimony. He states he went to Dr. Koch in 1931, whereas it was December 1932).
“In about two weeks, something like that, I noted that these little growths began to disappear. I would say in about six or eight months after that I could not feel them. They were gone. There have been no recurrences since then, and my health is pretty good.
“I work six hours on Sunday and twelve hours on Monday, Tuesday, and Wednesday. That is forty-two hours for the week. I am working that way right along.”
AN ANALYSIS OF THE REBUTTAL IN THE ABRAM JOHNSON CASE ATTEMPTED BY DR. FURSTENBERG
The rebuttal was contributed in this case by Dr. Furstenberg, of the University of Michigan Hospital. He gave an “opinion” that the growths might all have been removed by the cutting and cautery applied in this case. His “opinion” was that the growths that formed later were the scars from the cautery used to irradiate them. He never saw them so he did not know.
However, an examination of the facts shows that they deny the “opinions” given. Thus, in the first place, there were twice as many more growths formed when the disease returned than there were when the operation was done, and much wider involvement was evident when the Koch Treatment was given, than when the operation was done. The soft palate and neck glands had become involved and swallowing and speech were impaired. Therefore as cancer behaves, its seeds having spread to distant places and between the visible places that were touched up with the cautery, it was natural to observe growths develop where they could not be seen at the time of the operation, and where no cauterization was done. These growths could not have been caused by the cautery, since they came in places where the cautery was not applied. Since they were papillomata, they could only have been extension of the disease.
Dr. Wirth was also called upon to testify as to his “opinion” on behalf of the Federal Trade Commission. He gave the “opinion” that the new growths were inflammatory tissue resulting from the operation. However, the facts deny the correctness of this “opinion,” because the growths came after the operated areas were healed and after the inflammation had long disappeared. They were neither scars nor inflammatory reactions, but tumors of the papillomatous squamous cell type, readily recognized by their gross characteristics.
It should be observed, also, that the distribution of the new growths is exactly what takes place as the disease spreads, because the glands in the neck and under the jaw develop tumor masses, along with the appearance of the recurrent cancer in the mouth. It is evident; therefore, from the facts that the disease was made to spread more rapidly and become more malignant because of the “touching up” it received at the University Hospital. For as Ewing states on page 53, “There can be little doubt that the rough manipulation of cellular tumors in the excision of the growth, widens the field of infection by forcing cells through the vessels and tissue spaces.” Also, “Arising from the remnants of the original growths, recurrence is usually prompt, multiple, in the line of incision or nearby, and of the same type as the original growth or more malignant.”
A conclusive fact in the defense Testimony, which the Government did not even try to rebut was the fact that after the Koch Treatment was given, the recovery follows definite cyclic reactions peculiar only to the Koch Treatment. Mr. Johnson demonstrated those reactions very definitely and undeniably.
Thus, the nature of this disease at the time of the Koch Treatment is firmly established and a hopeless case of cancer of the mouth, stimulated to increased activity by inadequate surgery, became a permanent cure after the Koch Treatment. Friends spoke to Mr. Johnson recently and find that he remains in perfect health and is very grateful.
Hypernephroma, Metastasized to the Chest
THE CASE OF MRS. SHAW
A Paraphrase of the Testimony of Dr. H. E. Mantor. “Mrs. Shaw first saw me in 1917. She had a severe hemorrhage from the uterus. There was very excessive bleeding. This bleeding persisted for some time, and in June 1917, Dr. Jones, of Omaha, removed the uterus and found that a large fibroid tumor was the cause of the bleeding. She did not regain her health very well. She was a delicate little woman, and for a couple of years she wasn’t able to do her work herself.
“November 5, 1923, she developed an acute cystitis inflammation of the bladder. Examination revealed an enlargement of her right kidney. It was large enough so it could be palpated below the costal region or margin. There was tenderness on pressure there, and she had some pain in her back and on the right side. Microscopically, I found red blood cells in the urine, and granular casts in the urine, indicating a breaking down of the kidney cells.
“My professional diagnosis at the time was a stone in the kidney. I was in error, but that was my opinion at the time. In the fall of 1926, the attacks were much worse, harder, and more persistent than they had been. October 13, 1926, I was called out to their place, and she was having a severe attack of pain. I found her right kidney was greatly enlarged and was rigid clear to the crest of the ilium. I X-rayed the kidney a few days later, it showed an enlargement of the kidney and liver, and one of the mediastinal glands about the level of the aortic arch was enlarged to about the size of an egg. All this indicated a malignancy with a metastasis. That type of growth will extend by way of the lymphatics, and there was a lymphatic gland right in that position. At that time she weighed 108 pounds.
“I didn’t treat her until December 21, 1926. This was the first case I ever treated with the Koch Remedy, Glyoxylide. On the 29th, she was free from pain. January 5th, she was down to 99 pounds, but the right kidney had receded to the point where I had to reach up under the costal margin and the lower ribs to feel the lower part of the kidney. The liver had returned to its normal size. The patient herself felt a great deal of improvement. May 28, 1927, I took an X-ray again. The mediastinal gland was reduced to one-half the size it showed the previous time. The kidney and liver were still normal in size, and she had no distress from it. There were no abnormalities in the urine. The kidney was functioning normally, she was feeling well, and weighed 120 pounds. My diagnosis of the case was hyper-nephroma with metastasis.”
AN ANALYSIS OF THE REBUTTAL IN THE CASE OF MRS. SHAW ATTEMPTED BY DR. WIRTH
The rebuttal Testimony was offered by Dr. Wirth, and his favorite alternative to cancer was again applied, namely that instead of cancer the condition was infection. The kidney had turned into an abscess, and the enlarged gland in the mediastinum was also an abscess. Infections of such great extensiveness, as Wirth claimed this was, must naturally cause much fever, but Wirth says not. Yet, the amount of pus and fever produced depend upon the activity of the defense mechanism and when one is very active, so is the other. Thus, with this great amount of pus, we would expect the body to produce a high fever. In this case, fever was not present or at least noticeably high. It is also known that when a pyonephrosis develops from a hydronephrosis, or in ordinary English, when a kidney is enlarged by the blockage of the flow of urine, it will turn into an infected kidney or abscess, and must be removed. The severe pain and toxicity from the infection and the high fever demand drainage by large and deep incision through the back, as an emergency measure, and the removal of the infected kidney, besides. This was not necessary in this case, nor was it done. Thus, the “opinion” of Wirth is not in accord with the well-established facts. Nor would so extensive an infection wait from October 13 to December 21st of any year for active treatment. The patient would have been dead in days or weeks and would not last two months, without drainage of so great an infection. No medical treatment, not even oceans of penicillin, can cure such a case without the aid of drainage, so the one dose of the Koch Treatment showed its superiority over all other forms of medical treatment known today, if in fact this was an infection, as Wirth stated. But those who understand and write about kidney tumors agree with Dr. Mantor’s diagnosis, and so it is more likely that the disease in the kidney and in the chest were both cancer, as Dr. Mantor decided.
Massive Uterine Fibroma with Possible Malignant Change
THE CASE OF MYRTLE A. ROBERTSON
A Paraphrase of the Testimony of Mrs. Robertson
“About twelve or fourteen years ago I suffered from some trouble in my abdomen. I had a kind of rash on me and then I went to a doctor and he told me I had a tumor. I just felt miserable all over and I had kind of uterine hemorrhages. This had not lasted for very long. The first doctor sent me to Dr. Henderson. Neither of them treated me. Dr. Henderson had told me that I would have to have an operation. This was before Dr. Koch treated me.
“I went to Dr. Koch and some pictures were taken of me. The first one was in September 1930, and the second, at the end of 1931. (Ex. 171 and 172). At the time of the picture 171, Dr. Koch put me on a diet and gave me an injection. With the shot and the diet, the trouble in my abdomen seemed to gradually disappear. I felt better generally and the hemorrhages stopped and everything.
“There would be kind of reactions, but after it was all over I felt a lot better. I had two injections, it may have been three, but I believe it was two. I have been well since then, have gained weight and am much better.”
TESTIMONY OF DR. KOCH
(Photographs of this patient were introduced. They were Exhibit Nos. 171 and 172.) (Plate 33)
PLATE 33. These are “before and after” photographs of Myrtle Robertson. In the photograph above, taken before the Koch Treatment, the large, bulging growth that filled the lower abdomen and compressed its contents is easily seem, in the lower picture, after recovery, every trace of the growth had been absorbed, and the abdomen is normal.
“Mrs. Robertson was in pretty good nutrition, but she was rather hard of hearing for a long time. You had to yell at her to get her to understand what you were saying, I remember that. Then she had this large tumefaction in the abdomen, which was different from the ordinary fibroid in that it was fixed, and did not move as readily as a fibroid would, and it was not as smooth as the picture indicates, to the feel, at least. It looks pretty smooth there, but in feeling it, it was not so smooth. It was rougher and more lumpy, as it were, than fibroids would be of that size. On examination through the vagina, one found that the uterus had become this large mass and by examination through the rectum, one could feel that it was pressing the bowel very seriously and, no doubt because of the history of slow growth, had been compressing that bowel for some time.
“Yes, I believe that would be the cause for the constipation that she reported. She had to have her bowel movements fairly well liquefied to get by because the pressure, the squeezing of the anterior layer of the bowel to the posterior layer, was quite tight; that is, one had a hard job getting a finger up between the posterior wall and anterior wall of the bowel. The growth was a uterine growth; it was the uterus itself that had undergone this enlargement. Of course, in looking at her for the first time, one would not know whether she had a sarcoma or a fibroma, at the time I examined her at the start.
“She had three Treatments, December 2, 1930, May 16, 1931, and May 9, 1932. Between the first and the second Treatment she had a rather rapid disappearance of these extra portions of the growth, as it were, the lumpiness and the fixation, so that it began to resume the character more of a fibroma. It was movable then and subsequently was rather slow in disappearing. It took a couple of years and I gave her these other two Treatments to help it along, so my interpretation of that case is that here is a case of a fibroma that had undergone a malignant change.” (Paraphrased from the Official Court Record, pages, 5181 ff.)
AN ANALYSIS OF THE REBUTTAL IN THE MYRTLE ROBERTSON CASE ATTEMPTED BY DR. WIRTH
The rebuttal in this case was given by Dr. Wirth who disagreed with Dr. Koch’s decision that there was a “frozen pelvis.” Of course, the condition known as “frozen pelvis” is ascertained by feeling with the fingers the structures found through the vagina and the lower abdominal wall. The “opinion” witness is at a disadvantage, and should not hazard an “opinion” without the opportunity of examining for himself. Dr. Wirth suggested that “frozen pelvis” might come from infection, but the physician who examines the patient knows if infection is present from the history and general status of the patient, as well as, from the texture of the tissues, which are vastly different when infiltration are produced by malignant invasion than when produced by infection. Moreover the progress of the disease tells what it is.
An infected pelvis of such great extent, as the affected area in this case, would cause so much pain and fever that an emergency operation to drain off the pus would be soon required, and in the meantime, other anti-infection procedures would be needed. This is understandable by any layman who looks at a photograph of the patient when the Koch Treatment was given. A person with such vast infection could not run about town day after day. She would be bedfast, crying with misery every time she passed urine, or the bowels moved, and all the time in between.
Dr. Wirth testified also that a fibroid of this size would disappear spontaneously after the menopause. We know of no one who has ever seen such a thing happen. But if it would with the gradual let up of ovarian activity, the disappearance would he slow at first and increase in rate as the ovaries were completely atrophied, and no more secretion was present to stimulate its development or support its presence. On the contrary, the facts show that the disappearance was rapid at first and slow toward the last part of its dissolution. Thus, Wirth’s “opinion” again is not supported by fact or experience.
Absorption of a large fibroma of the proportions shown here would be nothing to take lightly either.
Terminal Recurrent Retroperitoneal Leiomyosarcoma
THE CASE OF BERYL F. CUMIMNGS
We wish to present two cases in this new edition of the book, which came about as a result of reading the earlier editions. Space does not permit more, although a great many have been reported to us.
The history of this case shows a father who died of cancer. She had eleven major operations at various hospitals beginning with removal of a tumor from the breast in 1929, a cancerous pregnancy in 1937 involving hysterectomy, and finally, the removal of a kidney in 1952.
These operations began in 1929, but the case became serious in April 1950, when she experienced considerable difficulty, because of a kidney block and subsequent infection. She underwent surgery under very capable hands and a large tumor mass was removed from the abdomen.
In 1952, difficulty returned and the malignancy attacked the Renal Pedicle, at the base of the left kidney. This made necessary the removal of this organ, because its arterial supply was involved. From tissues sent to Doctor’s Hospital in Seattle came the biopsy report (Path. No. 52-1706) with diagnosis from same as “Recurrent Retroperitoneal Leiomyosarcoma with invasion of Renal Pedicle Structures and Gastro-Hepatic Ligament.” The future was dim.
About three years later in July 1953, difficulty and pain struck again. It was discovered at the hospital that the malignancy had spread widely through the abdominal cavity and that it now completely surrounded the aorta. There was no surgical answer to this development, so the patient was sent home with a terminal prognosis. The biopsy from Doctor’s Hospital gave the diagnosis as “Recurrent Retroperitoneal Leiomyosarcoma.”
The husband of Mrs. Cummings writes: “It was just about this time that someone presented me with a copy of ‘The Birth of a Science’ and this person must have been a real friend to give me, the husband of the patient, so cherished a gift for I found out that the book was at that time out of print and irreplaceable. What it told me set me on a quest of inquiry into the facts.”
As a result the patient was brought to Dr. R. H. Barker, of Seattle, on a stretcher. She was given the Koch Treatment on January 8, 1954, and Dr. Barker intelligently explained the importance of food and diet and showed the patient a new way of living. He did not believe there was much hope to save Mrs. Cummings, because of all the adverse factors and the terminal prognosis made some months before at the hospital.
In about fifteen days after receiving Glyoxylide, the patient was off of all narcotics. Pain was not entirely gone yet, but it was bearable. At the end of six weeks, she was allowed to go home, a blessed event for her children and husband. By the middle of October, the full time housekeeper was only needed a half a day and by the end of 1954, she only came one day a week to do the heavy cleaning.
On Christmas Day, 1954, the patient entertained the entire family at dinner and by May 1955, she took an auto trip with her husband to visit relatives in the East, whom she thought she would never see again. The 8,5OO mile trip was accomplished without a bit of trouble or even tiring in the least. As this is written late in 1956, almost three years after receiving the Koch Treatment she remains in the best health she ever had.
Now let us look at the rather famous Judy McWhorter Case down in Texas.
THE CASE OF JUDY Mc WHORTER
85% Involvement of Cancer of the Liver In a Six Weeks Old Infant
Occasionally a cured patient, who received the Koch Treatment, breaks through the silence imposed on such events by the AMA and receives newspaper and/or radio publicity. They become famous. Such is the Case of Judy McWhorter. Here is a baby ill at only six weeks and declared hopeless for recovery after an exploratory operation at age 12 weeks. The operation showed 85% involvement of the liver. This was a most spectacular case of recovery. TIME magazine was attacking Dr. Koch and almost caused Judy’s predicted death because of the way this magazine prejudiced her parents from Dr. Koch, even though her family doctor could offer no hope.
This baby’s waist measurement at the time of the exploratory operation was about 32 inches! See the pictures (Plate 33A, B, C, D, E, F, and G). Most of these were taken in color to show the difficulty more clearly, but the black and white reproductions leave nothing to the imagination.
When the AMA cancer specialists met in Fort Worth, as is indicated in the affidavit following, one of them was Dr. Reimann of Pennsylvania, who had testified against Dr. Koch at the trial in Detroit. The conclusion of all of these experts was that Judy had cured herself in some unusual fashion, when most of them knew she had had the Koch Treatment! Judy’s pictures appeared in the paper, but the fact that the Koch Treatment had cured her was never mentioned.
Dr. Reilly visited with the McWhorter family on October 12, 1956, just a few months after Judy celebrated her 8th birthday. She has gone well past the five years usually set aside without a recurrence, the author had not seen Judy since she was two years old when she attended a convention of Koch doctors in Detroit. At the time, she was extremely active and he took Judy and his own daughter Donna (almost the same age) on several outings around Detroit. Little Judy’s activity was up to that of anyone her age. She was only too willing to show anyone who asked her scar across the abdomen received at the time of the exploratory operation when she was 12 weeks old. Her parents report her in fine health and getting straight “A’s” in school. Below is the Affidavit they made in June 1950.
Affidavit
“TO WHOM IT MAY CONCERN:
“In order to put on record the facts we know concerning the illness, treatment and recovery of our daughter, Judnita McWhorter, hereinafter referred to as just Judy, we make the following statement of our own free will and accord, without promise of or hope of any remuneration, and having previously received no remuneration of any kind.
“After a normal birth, Judy, before the age of six weeks, showed signs of illness. Her abdomen was enlarged, she was restless, and her face did not show the repose of a healthy baby. Her physician who was a doctor in good standing, a member of the American Medical Association, and a man whom we trusted and still hold in high esteem, could not find anything wrong with her until his check-up and examination at the end of her eighth week. At that time the doctor found her abdomen hard and much distended. During the period from August 20, 1948 to August 27, 1948 a tentative diagnosis of cancer was made and X-rays were given although the X-ray technician stated that it was hopeless to expect a recovery.
“By the time Judy was three months old the attending physician and another surgeon made an exploratory operation on Judy’s abdomen at which time a biopsy was made. The physicians reported to us that the biopsy showed a high degree of malignancy, which involved 85 % of the child’s liver. They told us that there was nothing that could be done to save Judy’s life; that we should take her home and make her as comfortable as possible for the few days that she could live.
“Her life expectancy was placed at 21 days. We were told not to remove the bandage from her abdomen lest the stitches burst out. It was the doctor’s opinion that the incision in her abdomen would not heal.
“For some days prior to this time Mr. Joseph O. Noah, a neighbor and old friend of Mrs. McWhorter and her family, had been advocating the use of the Treatment offered by Dr. William Frederick Koch, known as Glyoxylide. None of us had much confidence in this Treatment.
“When our doctor was consulted he assured us it was useless. He said he would not give it to his own child under the same circumstances, and that it would be an unnecessary and useless infliction of pain on the patient. He also made the statement that he would believe in the Treatment if he could see one case recover from the use of it where a biopsy showed positive malignancy.
“It was while we were considering this Treatment that Time (magazine) published its defamatory article about Doctor Koch, in the issue of September 6, 1948. This article was brought to our attention by both our physician and Mr. Noah. We found it very hard to take Dr. Koch’s Treatment seriously in the face of such criticism. Nevertheless when we had no other hope and since Mr. Noah made it possible for us to take the Treatment without immediate cost to us, we decided to try it.
“Dr. Koch’s Therapy was given by Dr. N. T. Mulloy, of Texas. The dose was injected into Judy’s hip on September 18, 1948. At this time and during the course of Judy’s recovery, Mr. Noah took a series of color pictures showing her progress. Previously he had taken two pictures at six weeks of age and before diagnosis of cancer. This series of pictures gives a good idea of her case.
“At the time the injection was given, Judy’s abdomen was so much enlarged that she could hardly breathe due to the upward pressure on her lungs. The circulation on the surface had greatly increased and she had a bluish cast from a diffusion of blood, in and just under, the skin. Veins under the skin of the abdomen were plainly visible. The abdomen was very firm, even hard. At the time the Koch Treatment was given, Dr. Mulloy expressed no hope of securing a recovery as he thought the case was too far advanced.
“Within ten days after treatment, Judy showed definite reactions, which raised our hopes. Shortly she began to pass large quantities of mucous with bowel movements. She also passed a large amount of water in the normal manner, sometimes requiring as many as twenty diaper changes per day. No medication was used after the injection of the Koch Treatment and only minor changes were made in the baby’s diet. Apple juice was substituted for orange juice, and Judy liked it. After the Treatment was given and until recovery was practically complete, only one doctor saw Judy. That was a doctor residing in Texas, who removed the stitches from the healed incision about the middle of October 1948.
“During the early days of the recovery process, Mrs. McWhorter reported to the doctor who had previously cared for Judy and who had advised against the Koch Treatment, that she was apparently getting better. He admonished the mother not to entertain false hopes. He said that it was impossible for a dose of any chemical to “destroy” such a large growth.
“On the other hand, Mr. Noah stated that the doctor’s remarks showed that he had no conception of how the Treatment was to work. He said one might as well say that a small match could not start a large fire and destroy a forest.
“Soon Judy began to gain weight and her abdomen rapidly reduced in size and became more soft and pliant, so that she could breathe better. The hard growth receded toward the lower right side. By December 25, 1948, she had a healthy and normal appearance as the pictures previously mentioned show, but some trace of the growth remained.
“Later, about May 12, 1949, I had her examined by a Doctor in Paris, Texas (Mrs. McWhorter told the doctor to make a thorough examination for trouble of any kind. He could find nothing, after which he was told of the baby’s former trouble and he could still find no trouble.)
“On November 11, 1949, Judy and her mother appeared before a group of physicians and surgeons especially interested in cancer that met at the Blackstone Hotel in Ft. Worth, Texas. While before this group, more than one doctor examined Judy and nothing was found wrong with her.
“Mrs. McWhorter states that a more surprised group of doctors would be hard to find when they first saw a rosy, healthy child rolled out before them after having read a clinical summary of her case.
“An account of this meeting with a picture of Judy and her mother was published in the Fort Worth Sun-Telegram. The piece was headed: “DOCTORS CONVINCED THAT LITTLE JUDY OVERCAME CANCER AILMENT HERSELF.”
“This in spite of the fact that all concerned knew that Dr. Koch’s Treatment had been given and that we gave it full credit for bringing about the baby’s recovery. The only excuse we can offer for this is that undue excitement might have been raised by a publication of the true facts.
“On February 18, 1950, both parents and Judy attended a meeting of physicians and others at Tampa, Florida. Here Judy was again shown to a group of doctors. These were most friendly to the Koch Treatment.
“Judy is now past two years old. She has shown a normal growth and development, normal mental development, and absolutely no abnormalities, that we are aware of. She is very active, mischievous, and friendly. She has had practically no illness after taking the Dr. Koch Treatment and recovering from cancer.
“Witness our signatures:
“Mr. O. McWhorter, Jr., Father
“Mrs. Otis McWhorter, Jr., Mother”
State of Texas . . . County of Parker . . .
Sworn and subscribed to me on the 28th day of June 1950.
Jim Bob Nation
Notary, Parker County, Texas
The wife of a prominent Christian Fort Worth publisher, who had herself been cured of undulant fever, went to talk with Mr. Noah and when she learned the name of the AMA physician-surgeon who did the exploratory operation of Judy, she discovered it was a neighbor. She called him on the phone. He verified that he had been Judy’s physician. He verified that the biopsy showed cancer of the liver. He is the doctor that told Judy’s parents that if he could see just one case of biopsied cancer recover with the Koch Treatment he would believe.
When the publisher’s wife asked him if he knew Judy had had the Koch Treatment he replied in the affirmative, but then he added that it was not responsible for the cure. He went on to say that in every 100,000,000 cases of cancer or so, there is one case, which recovers on its own, and Judy’s is one of these cases. The lady asked him if science observed 100,000,000 cases? Of course, there was no answer. There are not that many cases on record, since records began in order for the doctors to know that this was a pattern, they would have had to observe it at least five or six times, meaning observing 500 or 600 million cancer cases.
So, confronted with the facts known to his own conscience, this doctor refused to acknowledge the truth and rather used a wild story to show she made her own recovery. He told the inquirer that he would tell the world that he had made an error in his diagnosis rather than admit that the Koch Treatment had had anything to do with the cure of Judy McWhorter.
PLATE 33A. Judy McWhorter at 12 weeks with 21 days to live.

PLATE 33B. At 14 weeks showing exploratory scar.

No. III, Taken several weeks after Treatment
PLATE 33C. At 5 months of age.

No. IV, Taken a few weeks later.
PLATE 33D. At Christmas Time, 1948.
PLATE 33F. At four years.
PLATE 33G. Judy in school photo eight years after being given the Koch Treatment, September 1956.
Judy McWhorter as a young lady.


THE INTENSE SEARCH for a vaccine to counteract the polio virus has received national publicity for the last several years. Finally announcement was made amid much fanfare and acclaim that the cure for polio was at hand in the Salk vaccine.
Never before in the history of medical research has there been such a glorification of a medical announcement. Medals were handed out; Mrs. Salk became a sought after writer for women’s magazine and the tremendous work of inoculating millions of human beings was well underway.
It is too early to put a final stamp of approval or disapproval on the Salk vaccine. It is not too late, however, to review some of the things, which added to the confusion. Even as this is written, the Associated Press (10-8-56) carried front page stories about Dr. Albert Sabin of the University of Cincinnati who plans to give live polio virus by mouth to a group of volunteer prisoners at the Chillicothe, Ohio, Federal Reformatory.
An article appeared nationwide on July 6, 1956 giving information on polio from Dr. Theodore J. Bauer, the top health expert on this subject. One was clipped from the Arizona Daily Star of Tucson on the above date. The same subject was covered in some news magazines, etc.
In it Dr. Bauer says that among the nearly 30,000 polio cases of all types reported in 1955, about one-third “could not be identified in the laboratories as poliomyelitis.”
Later in the same article Dr. Baeur refers to this one-third as “non-polio viruses.”
Bear this one bit of information in mind that according to Dr. Baeur and the U. S. Public Health Service, whenever you read polio figures comparing this year’s (1956) cases with last year’s (1955), you must deduct one-third off the 1955 figures, which could never be identified as polio viruses.
One week later, the International News Service reported on July 12, 1956 (clipping is from Los Angeles Examiner, July 13, 1956) the following, and herewith the article is quoted in full:
Sometimes a doctor will point out that so many of a certain number of new cases in a given area were investigated and none of them had had the Salk vaccine. BUT, those given the Salk vaccine have been known not to contract the disease, while they carried it to others.
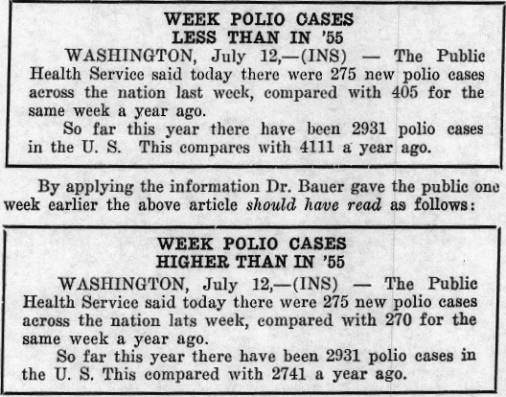
Whole families were stricken last year in this manner. Who can tell how many of those injected with Salk are carriers or not carriers of the disease while not getting it themselves?
Even the Journal of the American Medical Association in its issue of January 21, 1956, contained an article by Herbert Ratner, M. D., the Health Commissioner of Oak Park, Illinois, containing serious warnings about the entire production and distribution system of the Salk vaccine. Hardly any layperson read this article and possibly few doctors took the time to do so.
Dr. Ratner concludes his informative article with these lines: “Neither the public nor the medical profession was informed of these justified uncertainties, nor is it certain that we are yet being adequately informed. Finally, we should recognize that only one side of the ledger is being presented by the promoters of this vaccine. The price that has been paid and the risks that have been taken for the dubious results that have been obtained are not mentioned. The price that we have paid, and are continuing to pay, goes far beyond those known vaccinated children who have come down with poliomyelitis.”
Go to your public library reference room and see pages 231-232 of the JAMA for January 21, 1956, Volume 160, No. 3, for the entire article.
It is well known that the virus of anterior poliomyelitis is able to attack any portion of the central nervous system, but that it generally finds certain areas preferable for its development and destructive action. Therefore, polio cases conform clinically to certain types. It is also known that viruses change their characteristics quite easily. This fact is well demonstrated in the new “killer type” of polio that selectively attacks the vital centers in the brain stern and causes early respiratory paralysis. The symptoms of the bulbar type of polio have not been described satisfactorily so far as we can find. Among different patients a great variation of symptoms can be presented. There is, moreover, a periodicity in the severity of the symptoms during the advance of the disease that is worthy of consideration. This periodicity is also expressed in the decrease of their severity during their recovery.
It is well known that viruses, even more than ordinary germs, are subject to destructive oxidation. The Koch Therapy serves as an auto-oxidant to induce the destructive oxidation of the polio virus in the patients considered in this report.
The amount of recovery from paralysis depends upon the amount of actual destruction of nerve cell bodies that occurred in the spinal cord. Some cells are irreparably dead, but others appear incapacitated by the virus infecting them over a period of many days or years over which they can regain ascendancy, after the Koch Treatment. Thus, by a restored auto-oxidation of the normal type, these cells overcome the virus and regain good working structure. It appears also from Dr. Koch’s studies that the virus is able to inhabit the muscle, and that an attempt at walling off with diffuse or nodular fibrosis is the result. These, too, are found to disappear when the virus is overcome and the atrophied muscle regenerates and functions again in a major way. The amount of restoration of function cannot be predicted, but where the paralysis has existed only for a day or two, full recovery is often possible. Where it has existed for three years with marked atrophy, nearly full recovery is possible, and where it has existed for twenty years with extreme atrophy, the atrophy has been overcome sufficiently for good physiological activity. Good muscular legs were restored. The patient gets about as well as anyone without the use of braces or other contraptions. The case histories here given explain these observations.
A case of bulbar poliomyelitis with extensive paralysis is supplied in the Testimonies of Dr. David H. Arnott of London, Ontario and of Dr. Koch in the court record. He was treated in August 1936.
The patient, J. K., age 17, had been ailing for a few days before the paralysis set in. His chief complaint at that time was pain in his ribs on the left side, and some headache. Two days later the right leg became paralyzed. He was running a fever and was suffering much pain in the back, ribs, and head. The bladder failed to function and the paralysis started four days preceding our first visit. When first seen by Dr. Arnott and Dr. Koch he was semi-comatose, bloated, cyanotic, and both legs and arms were paralyzed. There was both respiratory and abdominal wall paralysis. The abdomen was greatly distended and flaccid. There was no respiratory excursion. If any breathing took place, it was too shallow to be observed and would have to be diaphragmatic. Yet, no breath could be detected, and he made a peculiar pain noise from time to time. The right eye was turned outward and the eyes were twitching. Swallowing was paralyzed, we learned later. He was given a dose of the combined polymers, and in ten minutes a respiratory excursion plus tightening up of the abdominal muscles was observed. They then catheterized him and gave colon lavage. They found that the whole torso was paralyzed, just as flaccid as a rag, the neck muscles too, for he could not hold his head up at all, as though he were under an anesthetic. The heart rate was very rapid and weak. All of this paralysis, excepting the right arm and legs disappeared within a few hours, and by morning he was able to swallow and talk. The cyanosis was gone, but still he appeared to be near death. After twelve weeks he could walk, but though the heart rate improved rapidly, every week on Sunday during the recovery the heart would go into a similar exhibition of tachycardia and weakness developed. This lasted a little over a day, and then subsided, to be repeated again the following seventh day, until the twelfth week had passed.
He still carried a residual atrophy, to some extent, of the right calf and hamstring muscles and the right transversalis abdomenils. He walks about, and can dance as well as anyone, but cannot climb stairs as well as a normal person. Otherwise, he is in good health.
Thus a widespread paralysis, which was terminating fatal at the very moment of receiving his Treatment, was quickly reversed, and the life was saved. Some of the paralysis that existed for over four days did not completely recover, but the rest did, and a useful, happy life with a minimum of handicap was secured.
Acute Poliomyelitis with Paralysis
In 1931, Walter Novikoff was two and one-half years old. He was carried into Dr. Koch’s office by his father. Both legs were paralyzed. For a day or two before this he had been crying, vomiting, had fever, and complained of pains in his legs. Then he could not get out of bed in the morning or stand up. It was found that the knee jerk was absent and he could not stand. His legs were not under control and were attacked by a flaccid paralysis and foot drop. Examination also showed irritation of the spinal cord. He was very ill. The paralysis had lasted over twenty-four hours. The polymers were injected intramuscularly. In about an hour he unconsciously swung his legs, and, on testing, could control them. He was carried home, and within twenty-four hours recovery was complete. No sequelae remained from the attack. The paralysis was fully overcome and his health good. He is now a big strong boy of eighteen years and perfect musculature, weighing 180 pounds.
Polio with Paralysis
REPORTED BY MRS. NOVIKOFF, THE MOTHER
“I took my son, Walter, to Dr. Koch when he was two and one-half years old. He had been playing the night before, but during the night he did not sleep and cried, and when he got up he could not walk. I did not take his temperature, but felt his forehead and thought that he had a temperature. His leg was still sore, so the next day we took him to Dr. Koch’s office. My husband had to carry him because he could not stand.
“Dr. Koch gave him an injection in the leg. We were in the office about an hour, and soon after he had had the shot he wanted to get off my husband’s lap onto the floor. He could stand a little, but we carried him to the car and kept him in bed that day. The next day he was up and playing. That was the summer of 1931 or 1932.”
Acute Poliomyelitis with Paralysis
THE CASE OF ROBERT LAWHEAD
Paraphrase of the Testimony of George Franklin Smith, M. D.
“Robert Lawhead was eight months of age when I first saw him. He was having convulsions and fever of 99 degrees. He had also been vomiting. The child would draw his hand up to his shoulder. The eye turned toward the side of his head so that the dark part was not visible. The face muscles twitched and the foot drew up. This convulsion stage lasted several days, and was followed by flaccid paralysis of the muscles of the right side. He became limp. When he was pinched there was no response. Neither motion nor reflexes could be elicited.
“I diagnosed the case to be infantile paralysis, and gave a dose of Glyoxylide. Improvement was gradual, and at the end of a week he was fully recovered. Today the child is eight years old, and no ill effects are present.”
Acute Poliomyelitis with Paralysis
THE CASE OF THE INMAN CHILD
Paraphrase of the Testimony of Dr. Michael Rabe
“The Inman child was ten years of age. He complained of headache and pains in the legs and back, and stiffness in the neck, with a temperature of 100 degrees. On September 8, 1941, this child could not move his hands or legs, and complained of pain in the back. He had no reflex action, except in one knee, which was exaggerated. Later on, this knee showed no response. This leg had also become paralyzed. A Kernig test was performed. The diagnosis was infantile paralysis. The Health Officer was called in, and he confirmed the diagnosis of infantile paralysis. I believe the child had had the disease from six to eight days by the time he was treated.
“He was given an injection of polymers on the 13th and again on the 18th. On the 14th, he felt better, on the 15th, less pain and could bend leg better. On the 16th, there was less paralysis. The child gradually improved and could go down stairs. Recovery did not require more than two weeks.
“At present he is in normal condition.”
Acute Poliomyelitis with Established Paralysis
THE LOMAN ATKIN CASE
Paraphrase of the Testimony of Dr. Wendell G. Hendricks
“Loman Atkin lives at Porterville, California.
“Loman was examined by me on the 4th of February, 1945. The first I knew that he was ill was about 8:00 or 9:00 o’clock that morning, when I received a telephone call from his mother in Porterville telling me of her boy’s symptoms. I anticipated a severe condition, and I told her to bring him to Bakersfield by ambulance, as I felt the case was a contagious one. I thought it was infantile paralysis (anterior poliomyelitis).
“The mother brought the boy to Bakersfield in an ambulance, took him to his grandmother’s residence, and as soon as he arrived she gave me a call by telephone, and I went down to this grandmother’s residence and examined Loman.
“It was between ten and ten-thirty when I arrived, and Loman was screaming with pain. You could hear him outside. In fact, when I talked to his mother over the phone just before coming down, I heard the boy screaming over the phone, so I immediately went down.
“The examination revealed this boy to be in a very painful condition; his neck was rigid, thrown back; he assumed a very marked extended position; his legs were paralyzed from the hips down, because I examined them and asked him if he could move them, and he could not.
“He had been ill for approximately twenty-four hours or more. As I recall, his condition started with a gastric upset, and it progressively had gotten worse until he developed these severe headaches and pains in his arms, legs, and in his back, which he still complained of, and very intensely so, during the examination.
“I diagnosed the case as anterior poliomyelitis on the symptoms I observed, and to confirm my findings, I did a spinal puncture, and the spinal fluid came out under forty millimeters of mercury pressure, which is extremely high. I withdrew only a few c.c.’s for the laboratory test to rule out meningitis. The test findings were consistent with polio and ruled out meningitis.
“To do a spinal tap, we prepare the back with an antiseptic, and then insert a spinal needle in between the vertebra into the spinal canal, and out through that needle comes the spinal fluid. Normally, the fluid will come out under a pressure of about eight to ten millimeters of mercury, which is normal, at a slow drip; but Loman’s shot out, and the pressure reading on the monometer was forty.
“That is a diagnostic feature of polio. I asked Loman, after the withdrawal of the spinal fluid, if he felt any better. He said, ‘No.’ In fact, he was very restless and kept hollering with his headache and the pains in his legs. We waited a half hour to see if there would be any relief. There was not any relief. So, I injected an ampoule of the polymers intramuscularly, and I instructed the mother to please keep a reading of his temperature about every hour or two throughout the rest of the day, and that I would cheek on the boy later on in the day.
“As I recall, this injection was given at 11:00 A.M., and the temperature at that time, just previously, was 104.6 degrees, which is very high, and which goes right along with the polio. His pulse was 128.
“At 6:00 P.M., I checked him again, and that boy could move those legs, about as well as he ever could. There was no paralysis. His neck had become limber and the whole examination was normal. His temperature had returned to normal. In fact, I think it went just a little bit below normal.
“I checked with the mother again the next day, and that night, after I had left, Loman had eaten a slight supper and had wanted to get up. His mother would not let him. But, the next morning he had gotten up and had walked unassisted to the bathroom.
“When I found that out, I instructed her to please keep him in bed, because I did not know just what the future results would be, and I wanted him kept under strict surveillance. I thought that, having an acute infection of that nature, it would not be wise for him to get up immediately on general principles.
“I saw him again on Wednesday, and at that time the boy was dressed and ready to go home back to Porterville. I had told them that he could go Wednesday if he was all right. He was all dressed and raring to go. He walked out to the car and got in just as normally as anybody.
“From that time up until the 18th of February, 1945, there was no recurrence; there was no recurrence of that fever, paralysis, or any of the symptoms whatever. This boy was perfectly normal, although I did have him stay in bed from the Sunday I treated him until the following Sunday, just for good reasons.
“On the 18th of February he had a slight attack of chills and fever, which lasted, I believe, about three hours, and after that the boy was perfectly normal again.
“The mother did not understand why these chills and fever came up and then went right away, but it left the boy with no other symptoms and immediately disappeared. I interpreted this occurrence as a third week reaction from the Treatment, a usual event in many cases.
“My diagnosis in Loman’s case was that of an acute condition. Within my experience and by my knowledge, this condition was a progressive condition; one that would grow progressively worse, definitely. I regarded the situation as one of emergency. That accounts for the fact that I administered Dr. Koch’s Treatment so quickly.
“Then, later on, in April, Loman’s two brothers came down with mumps, and they were very ill. They were sick for about a week. Loman took the mumps. He swelled up just a little bit, and in twenty-four hours he was completely normal, and he had no recurrences; did not even stay in bed more than twenty-four hours.
“From that time until this, on repeated occasions, I have seen him, and there has been no recurrence whatever of the polio symptoms.”
THE MOTHER’S TESTIMONY
“My name is Mrs. Ardis Atkin, and I live at Porterville, California. I am the mother of Loman Atkin.
“I was with Loman during the illness described. I personally observed the illness.
“He came to me about five o’clock in the morning, and he appeared to be in some distress with his stomach. He informed me that it was hurting, but I have three other youngsters, so I thought nothing of it and told him to go back to bed. But he seemed to have a slight temperature. I lay there, though, and heard him crying and moaning a little bit. And then later I got up, about seven o’clock, and he seemed to be in more distress, and I noticed about nine o’clock he appeared to be in much more pain. He was complaining about his head, it was aching quite badly. And I also had taken his temperature. I keep a thermometer in the house at all times, and I noticed that the temperature was rising, and it seemed that it was doing so rather fast, from five in the morning until nine was not a very long period of time. There were a number of polio cases in our locality at that time, and as this pain started to spread into his arms, I became sort of alarmed and thought of polio immediately.
“That was Saturday of the first week in February, 1945.
“Between nine and ten o’clock, sometime right along in there, this pain spread into his arms and his complete head, the front and back; his muscles started jerking, and I prepared a tub of rather warm water for him, and picked him up and carried him in there, and, of course, that relaxed him, and he seemed temporarily relieved. But it would seem to come back. I did that about three times, and then I was exhausted and I put on the hot fomentation. I did that that morning, but it was not long until it seemed that he did not have much relief. The pain just continued on.
”That Saturday the temperature rose to 104°, and it seemed to stay approximately that temperature the remainder of that day. And, of course, he screamed with pain. That afternoon it was frightful, and he was looking very bad. His eyes were glassy, and the pain did not seem to ease at all. That night was very bad.
“We had information regarding Dr. Hendricks, and we acted on that information. We engaged the ambulance and took the child sixty miles to Bakersfield by ambulance. We handled him very, very, carefully because he was in such severe pain and could not move his legs. We took him to my mother’s home in Bakersfield, where Dr. Hendricks attended him. I was present when Dr. Hendricks examined Loman and injected the medicine. I remained with Loman after that Treatment.
“I observed the developments after that Treatment. The doctor requested that I keep a chart of his temperature that evening, and it was 104.6° before the Treatment, and it steadily went down. Every time I took that temperature upon the hour, it was a little bit less than the reading previous, and by night, sometime in the early evening, it was sub-normal; a tiny bit below normal. I do not remember the exact temperature. He moved his legs slightly in the early evening, and he ate food. He appeared to be in much less pain during the afternoon, and he slept that night.
“On observing Loman the next morning, which would be Monday morning, he appeared to have gone through an illness, by his face, rather pale, but he was not in pain from all appearances. He got up and walked to the bathroom, and he wanted breakfast. He was hungry.
“I have been with Loman constantly since that illness. I have observed him to be a normal and healthy boy.”
PARAPHRASE OF THE TESTIMONY OF LOMAN ATKIN
“My full name is Loman Elwood Atkin, and I live at Porterville, California.
“I feel all right. I play baseball and football. My daddy is a foreman on an orange ranch. I help pick oranges and run little errands from the shop to the cow barn. I climb trees.
“I was sick two years ago. I had pain at that time. It started in my head and went into my arms, and in my back, and in my legs. My legs hurt badly. I could not move my legs while I was sick. I first felt sick at five o’clock in the morning. I got up and went and told mother that I did not feel well. Mother put me to bed and she thought it would be all right. I did not go back to sleep. I stayed in bed the rest of that day. I was sick; the pain got worse. Mother went and got a hot tub of water and gave me a bath and put me back to bed, and then did the same thing over again, and she got tired and gave me hot fomentations. They helped my pain a little bit. Then the pain came back. I stayed in bed that day.
“At nine o’clock the next morning, mother got me up and put me in the ambulance and took me to Bakersfield to my grandma’s residence. There I saw Dr. Hendricks. He went and pulled spinal fluid out of my back and then he gave me an injection in the arm. I do not remember now how I felt after the injection. I felt better late that Sunday afternoon. I tried to move my legs and could move them some, a little bit. Late that Sunday afternoon, I got hungry and had some supper. That Sunday night I slept.
“Monday morning when I woke up, I wanted to get up and walk around, and mother would not let me. I did get up to go to the bathroom. Then I went back to bed.
“I can run now and can climb stairs. My legs feel about the same as they did before I was sick.”
AN ANALYSIS OF THE REBUTTAL OF THE LOMAN ATKIN CASE ATTEMPTED BY DR. DONALD COOK YOUNG
This rebuttal of an “opinion” witness shows the danger of “opinion” testimony, because it actually distorted the facts upon which the diagnosis was built, and gave highhanded “opinions” contrary to common, everyday, knowledge among both profession and laity.
If the witness were present when the examination was made or had participated in it, he would not have made the following erroneous statements.
(a) He stated that careful examination to test the ability of the patient to move his legs was not done. He said that the absence of reflexes was not determined so the presence of paralysis could not have been ascertained. The history shows that these statements are false. The knee jerks were absent; passive motion and tests of ability and inability to perform active motion were made. The patient was not simply told to move his legs but when commanded to make motions of his legs the power of the various muscles to contract,—that is, both flexor and extensor contractions were found to be absent. Moreover, the history shows that the patient was unable to use his legs at all, to move them in bed or to stand on them. He was not even able to move his toes.
This state of flaccid paralysis lasted over twelve hours before the Treatment was given and continued about three hours afterwards before movement set in. The improvement was very rapid; complete restoration of motion came within twelve hours. Fairly good motion was had in five hours.
The witness stated that the patient was sitting up when the spinal puncture was made. This shows his lack of comprehension of the case. The patient was placed in a sitting posture while lying on his right side in bed; that is, he was placed on his right side and his legs flexed at the hips so that he was given a sitting posture. The stiffness of the back muscles and those of the neck, the witness had to admit, is characteristic of polio. The witness denied that it would be characteristic of polio, in this case, because it was too pronounced.
(b) The witness stated that the spinal fluid study did not confirm the presence of poliomyelitis. This is not true because the high pressure of the fluid as occurred in this case is characteristic in poliomyelitis. It may occur in meningitis also, but the cell count and other characteristics of the fluid showed it could not be meningitis and thus, the only disease that remained that could produce the paralysis observed and possessed this spinal fluid was poliomyelitis.
Other diseases were thereby ruled out. The witness stated that it is quite unlikely that a patient with 104° fever would have polio. Of course, this is absolutely untrue since polio is no longer an obscure disease. This high temperature range is known to be very common in the most serious forms of the disease where the paralysis is progressing up the spinal cords. This is the type that proves fatal.
The witness also stated that pain is not an outstanding symptom of patients with poliomyelitis. Such a blunder requires no discussion.
Altogether the expert, Dr. Young, was not able to deny the facts by claiming that the changes were either too pronounced or not well enough observed to make a diagnosis. Even the mother was able to make the diagnosis hours before Dr. Hendricks saw the patient.
Chronic Poliomyelitis with Paralysis and Atrophy of Three Years’ Duration
THE CASE OF MYRNA ROBINSON
Paraphrase of the Testimony of Dr. Julian F. Baldor:
“Myrna Robinson was brought to me in December 1943. She had had this infantile paralysis for three years. At the time I examined her, there was complete paralysis of the left leg and foot, with marked muscular atrophy. The muscle was gone and she had no power of movement of the left foot. There was contracture of the one toe of the same foot.
“The history of the girl was as follows: she was healthy and normal until she was stricken with a fever and a cold in the chest. After this receded, the left leg was paralyzed. She could not move the leg, and gradually the muscles disappeared.
“She had been down at the Warm Springs, Georgia, Sanitarium, but they discharged the patient without treatment, believing her beyond help. However, they put her leg in a cast for two months, and she also used a brace on the left leg to support the foot. The brace caused too much discomfort and gave no help, as the leg was too weak to use it, so the family discontinued its use.
“My diagnosis was poliomyelitis resulting in muscle paralysis and atrophy.
“It was the 11th of February, 1944, when I gave her the Treatment. Since the injection, she had two reaction periods of pains starting in the back of the head, that spread down the spine and involved the left leg, which was affected with the paralysis. I noticed the regeneration of the muscle in the left leg between examinations, and the foot that was completely loose and uncontrolled, is now perfectly and normally controlled by the girl, without wearing any shoes, and the retraction of the toe that was completely retracted, is now straight and normal. She is able to play like a normal child, and the atrophied leg has developed to be as good as the normal leg. All of this improvement took place in a few months after the injection. It is really miraculous. She does toe dancing now.”
Chronic Poliomyelitis with Paralysis and Atrophy of Twenty-one Year Duration
THE CASE OF MRS. VIOLET NICOLA
Paraphrase of the Testimony of Dr. Wendell G. Hendricks
“Patient, Mrs. Violet Nicola, lives at Bakersfield, California.
“Mrs. Nicola first consulted me on the 5th of April, 1943. She was twenty-three years of age. History, infantile paralysis at the age of eighteen months, twenty-three operations, and fifty-four casts; operations meaning surgical operations. Wore braces on both legs up until three and one-half years ago. Now walks on crutches dragging the right leg, which has a brace on it. Migraine headaches. Both legs on this examination of this girl were markedly atrophied.
“There was very little muscle at all on the right leg. The circumference around the calf was four inches. There was a contracted condition of both legs. The right leg was worse than the left; spastic, no relaxation. She was brought into the office by her husband, who carried her in and set her down, and I examined her. When she stood up she had to be held up by her husband; she could not stand alone. She was in a miserable condition, markedly underweight. Her weight was eighty-nine pounds at the time. She was very sick, very ill, and discouraged, and felt that she was doomed; never would walk normally. She ran a little temperature, about 99.6 degrees. I did not know what to do with that type of case, not having had experience with chronic polio cases at that time, and I explained to her the only thing I could do was to use Dr. Koch’s medicine. I explained what it was, what it might do for her, but I did not guarantee it. I did not know what it would do, but if she was willing to take it, I was willing to give it. She was willing. Two days later, I injected an ampoule intramuscularly. It was April 7, 1943. On June 8, 1943, approximately two months later, I could see a development in the calf muscles of the right leg especially, and there was motion. She was beginning to move that leg, and she could stand up by herself. The braces were off. She could walk unassisted around the room at that time. On August 13, 1943, she had a reaction of chills and fever, and with that reaction, she had a headache. Since that reaction of August 3, 1943, the patient had complete control, absolute complete control and power of both legs. She walked absolutely unaided with no crutches or braces. The muscles had developed, the cramps had ceased, and her weight had increased. Her outlook was wonderful at that time. In fact, she asked me if it would be all right if she adopted a baby and I told her if she could take care of a baby it was perfectly all right with me.
“On June 12, 1944, she had another reaction, and had some pain in her right foot and thigh. She was given a manipulative treatment on that day to relieve the pain present. She complained of no appetite. She had some fever.
“On June 16, 1944, she did not have any appetite, and some migraine headaches were persisting, and I gave her an injection of Vitamin B complex intravenously. I repeated that on the 21st, the next day, and again on the 23rd to give her an appetite. On the 23rd I also gave her another of Dr. Koch’s injections, and this time I did not do it principally for the polio, or the after-affects of polio alone, but I thought it might help the migraine condition she had.
“On September 8, 1944, she was given another manipulative treatment for her headache, and on September 11, 1944, she was given another injection of the Vitamin B.
“Now I forgot to say that in the beginning of the Treatment her right leg was an inch and a quarter shorter than the left, and she had to have her shoe built up on the outside, both heel and sole, one and one-quarter inches, in order that when she walked she would walk level.
“Now, on September 11, 1944, she had to build her left shoe up only one-sixteenth of an inch in order to compensate for the right leg.
“On November 11, 1944, she was given an intravenous injection of Vitamin B and calcium for a general tonic effect for lack of appetite.
“On November 14, 1944, she was given another injection of Dr. Koch’s medicine, and her headache was bad on that particular day, and she was given a headache powder called Saguinaria.
“Now, the patient has recovered from the paralytic condition. At the present time, as compared with four inches on the right calf, the measurement is now ten and one-half inches; as compared with ten inches previously on the left calf, it is eleven and one-half inches.
“Of course, most of the activity took place in the right leg, because that was the worst leg. There have been no recurrences of any cramps or the contractures that she had. She is able to run up and down stairs, and walk or run about like other normal people.”
It is difficult to interpret this restoration, unless the explanation of Dr. Koch’s is valid, that there is a symbiosis between the virus and nerve cells resulting in the paralysis of the cells so affected, but not their death, and with restoration of adequate oxidations, the functional mechanism is re-established, and as a result of such oxidations, the virus is destroyed. If this Theory is true, then the whole Koch Hypothesis, regarding energy transferred to the parasitic virus via the fluorescence of the toxin it employs is also true, and the nature of the auto-oxidations of function and the induced oxidations of immunity of this natural order appear reasonable. At least, this Theory seems to be substantiated by the behaviors observed in these cases, and in the cancer cases reported in this investigation. The restoration of the immunity and protective function of the white blood cells, mentioned here, are also supportive. In fact, we have a new philosophy covering the field of pathology and medical practice, which explains the unknown to date, and at the same time offers the curative agent. The utility of the entire conception is thus established.
TESTIMONY OF VIOLET NICOLA
“My name is Violet M. Nicola, and I live in Bakersfield, California. I was not born there. I lived there approximately twelve years. I have heard the Testimony of Dr. Hendricks, just given.
“For some time I suffered from a paralysis. I was stricken at eighteen months of age. I am twenty-six years old at present. From my earliest recollection, I was not able to walk. From the time I can remember, my legs were of completely no use to me at all. I was in bed practically all the time, except when I was lifted out. I could not stand up. I underwent treatments for these handicaps. I can remember I had twenty-two different surgical operations from the time I was six until I was sixteen, and then I had one other several months before I was twenty, which made twenty-three operations altogether.
“I remember most definitely the casts, first. Several of them were body casts that started under my arms, went completely down my body and down to my toes; and then some of them went from my hips down; and some went from above my knees down. The number, I could not tell you. These were casts. The steel braces that I had were rather iron, I believe, and there were iron bars up both sides of my legs, and the first ones I remember were above my knees and strapped to my thighs.
“I could not walk unassisted at the age of ten years.
“I could not walk unassisted at the age of fifteen years.
“I could not walk unassisted without braces at the age of twenty years.
“I could not walk unassisted four years ago.
“The way I got around, if I did get up, and when I did, I walked on what I would describe as three point walking. By that, I mean my crutches were two points, and I was a third point. I literally dragged myself, swung between the crutches.
“From the age of twenty until I was twenty-three, I certainly did notice a change. It seemed as though, instead of going forward, I was getting worse. I started dragging my legs again and nothing seemed to go right with them. I could not work them right, and they were, I thought, just getting useless to me again. About that time we got information regarding Dr. Hendricks. My husband took me to Dr. Hendricks as a last resort, we thought.
“Dr. Hendricks gave me a Treatment. He first explained to me the nature of the Treatment. It was in the first week of April 1943 that he treated me with the Glyoxylide.
“After I had the Treatment, within three weeks, I removed my brace, and discharged my housekeeper, who I had full time before. I did my own work and I made my visits to the doctor alone. I walk better now than I did then. I had three Treatments of Glyoxylide.
“I am now married. I met my husband in an ambulance. He was the driver and I was the patient. I have an adopted baby girl. She is two years and four months old, and she is a wonderful baby. I care for her personally, with the exception of when I work. I do my own housework and I am a stenographer and bookkeeper in a department store. I am a member of the American Credit Women’s Association and of the Bakersfield Women’s Club. I am Assistant Secretary for the California Auxiliary Highway Patrol, and I am also Secretary to our Kern County Kennel Club.
“I have not had any other treatment than vitamins, except Glyoxylide.
“Before I went to Dr. Hendricks, I was not able to exercise my limbs.
“My ability to walk today, compared with that of one year ago, is almost perfect. It certainly has improved. I can dance and I do dance.
“My limbs have changed in size in the last three years, definitely. My right leg has extended one and one-fourth inches, and both legs have grown inches in circumference.
“I wore braces all my life until three or four years ago. I do not wear braces now. I do not wear crutches or carry them now, whereas I did. I wore specially made shoes, but I do not now.
“When I first went to Dr. Hendricks, I weighed eighty-nine pounds. Two years ago, 119 pounds. My average weight is now 113. I would like to weigh a couple pounds more. I feel perfect now. I am extremely happy.”
Special Note: This Nicola case was one of the most interesting of the many presented by Dr. Koch’s defense attorneys in the 1946 Trial. For five weeks previously, the Detroit newspapers carried stories every day boosting the Government’s side. The defense began on a Thursday. At once all stories about the trial were stopped. The writer called the editor of what could be termed the “fairest” paper in town. The only excuse he received was that the Testimony was now technical and scientific and thus, not interesting to the general public. You have read the type of marvelous Testimony being given during this time. Of course, the fact that the yearly cancer drive was on . . . looking for a treatment for cancer, and the fact that Federal Court Testimony of countless recoveries, would have made the drive look insincere, if the papers carried the defense stories, possibly had much to do with the fact that the local papers refused to print the Koch side of the trial. Dr. Reilly)
AN ANALYSIS OF THE REBUTTAL OF THE NICOLA CASE ATTEMPTED BY DR. DONALD COOK YOUNG
The rebuttal in this case was that exercise of the muscles was what brought about the development and restoration of function. This is contrary to the facts because the patient could not use her muscles for a period of over twenty years that is, from the age of 1.5 years to the time she received the injection from Dr. Hendricks in April 1943. It took still several months after the injection before she could move them well, but she made the same efforts to try to move and use her muscles before the injection as she did afterwards. There were twenty-one years of a controlled period in which she had plenty of time to develop her muscles and overcome the paralysis and just as much incentive to do so as after she had received the injection. It was only a matter of a few weeks after she had the injection that the muscles started to regenerate and work.
It is also important to note that she had the characteristic reactions of fever, grippiness, etc., that go with the Koch Treatment and characterize the recoveries obtained by this Treatment and no other.
Any decent citizen will deplore the insulting attempt of an “opinion” witness to give such Testimony to rebut this case; it shows how depraved some of our Federal Court attorneys can be. Please read the Testimony of the witness and Dr. Hendricks’ again.
Chronic Poliomyelitis In a Pekinese Dog with Paralysis and Atrophy
SUBMITTED BY DR. B. J. MYERS
“This Pekinese dog gave birth to puppies in May, 1943.
“I first saw her August 12, 1943, with a partial paralysis of hind leg, symptoms of extreme nausea, and high temperature. By August 15th, there was paralysis of tail and other hind leg, in the following week she was completely paralyzed—four legs, tail, and vocal muscles. Muscles not affected were the neck and those of mastication. Abdomen was completely relaxed, and the high temperature persisted. This condition lasted until December 15th. During this time, she was given supporting treatment. Her colon was completely paralyzed, so that the feces had to be expressed mechanically. Prior to the injection, the legs and other muscles had completely atrophied and had started to contract and distort. The tissues of the legs were hardened on the verge of ossification.
“On December 15th she was given a Treatment of Koch’s 1:4 Benzoquinone. Twenty-four hours later the tail was curled, and in a natural condition; previously, it had been completely paralyzed and straight. Forty-eight hours later the dog could stand, and when supported she was able to move her legs. Three days later the dog could rise, and walk across the room. At present she is in a perfectly normal condition.
“There was a severe polio epidemic at the time in Oklahoma City, and one of the children next door, who played with the dog, was down with polio at the time, and just before the dog took sick.”
T APPEARS that the Koch System is the first chemotherapeutic achievement whose use is followed by an increase in the efficiency of the leukocytes instead of injury to them. The more efficient the function of a tissue is found to be, the less of that tissue is needed to accomplish a given piece of work. This holds also for the leukocytes and it is well known that as the toxicity of an infection increases, the greater is the stimulus to the production of leukocytes and the greater the number of these cells that appear in the blood and at the sight of the infectious focus, especially when their antitoxic action fails. Moreover, in some persons the production of efficient leukocytes is so poor that infection can go rampant, neither being walled off at its focus, nor burrowed to an exterior surface to be discharged. In such instances a Treatment is needed to give the leukocytes and the tissues that generate them the energy they need for effective function.
When such Treatment is effective, leukocytosis will be sufficient to bring about successful burrowing and drainage when needed, and exert adequate anti-toxic action to overcome the stimulus to leukocytosis. Pus will then diminish rapidly. The Case of Dr. Kolisch’s son illustrates the first achievement. The Case of the Reeves boy whom Dr. Andrews testified about is another illustration. In this hopeless fulminating case not only had the double pneumonia gone chronic, but the kidney infections, and the heavy infection of the blood stream with Staphylococcus aureus cleared up quickly and completely, and an uncontrolled osteomyelitis of the tibia was localized; the dead bone was walled off, and burrowing was started to the surface so that the surgeon could easily locate and clear out the debris. True permanent recovery followed, instead of death or invalidism, the usual chronic sequelae of osteomyelitis where the infection persists and healing is never completed.
The Pennock Case gives a measurement of increase in efficacy of the leukocytes in helping to remove the toxic stimulus to leukocyte formation. Immediately after the Benzoquinone was administered, the white blood count dropped at a rate of 3,500 cells per day towards normal and at the same time, recovery from the bowel obstruction, from the pain, inflammation, and fever, progressed with equal rapidity. Toxicity thus decreased with the drop in leukocytosis.
The Case of Mrs. Peabody reported in the Testimony of Dr. Wendell Hendricks presents another example of regeneration of efficient natural immunity. This Testimony established the quick reversal and recovery after a dose of Glyoxylide from an acknowledgedly incurable and far-advanced progressive bronchiectasis. This case also demonstrates the dependence of an allergic condition, asthma, upon lung infection and shows that removal of the allergy progressed with the disappearance of the infection. Thus, Dr. Koch’s working Hypothesis is again substantiated by fact.
There is also the Testimony on the chronic infection of the temporal bone of Dr. Loeffler’s daughter that would not improve under seventeen years of continuous care by the best experts obtainable. Yet after the Koch Treatment the disease process was quickly reversed and brought to gratifying recovery with redevelopment of some of the injured ear structure so that some of the hearing function was restored. In this case the whole life was changed as a result of the restored health. The Testimony of Dr. Woodruff about his son is analogous and also very instructive.
In the Case of Major Nobre every joint in his body was fixed immovably. The bones were grown together by scar tissue, which had developed to wall off the infection. A dose of Benzoquinone solution was followed by disappearance of the infection amid absorption of the scar tissue, which doubtless was no longer necessary as a protective measure. The joint surfaces that had been replaced by scar tissue were regenerated and motion was restored to 95% or so of the original normal.
Many other cases of infection could be abstracted from the Testimony. They were offered as proofs of the successful protection that quickly results after the administration of the natural type of auto-oxidants in stepped-up form. Until recently, such recoveries were too wonderful to be understood or accepted, but now that the beneficial work of penicillin has become widely known, it will be easier to appreciate the even greater efficacy of the natural immunity process of animal tissues. That the animal body has in its tissues a more efficient system of protection than can be borrowed from the mold, Penicillium Notaturn or its relatives, has just been demonstrated by Dr. Sperti, and reported in the lay press in 1947. He used Staphylococcus aureus as the infecting agent and brain extract as the protecting material, 100% protection was secured. This compares well with the protection secured by the Synthetic Natural Immunity Antitoxins we are discussing when used in human beings. Dr. Koch reported on this natural immunity as residing in heart and brain lipoids as curative in cancer, 30 years ago. His report was made in the Medical Record of New York, October 1920. Geiger and Conn have demonstrated just recently, also, that compounds containing the conjugated system of Carbonyl and ethylene are curative against these infections when present in certain compounds thus, confirming Dr. Koch’s publications of the past and the Testimony given in his various Federal Trade Commission and Federal Court Trials. Many other such publications are being made now, including the work of Warren, and that of Wesley and Rusch, which show that such structures cause the inductive oxidation of cancer producing poisons in confirmation of Dr. Koch’s teaching and Testimony.
The essential activity of Koch’s System was well demonstrated in animal and test tube experiments. The work on dairy cows with the Koch Treatment as detailed in the Testimony of the Ministry of Agriculture of the British Columbia Government, and the University of British Columbia, which demonstrates the efficacy of auto-induced oxidations in infectious diseases that do not respond well to mold products or sulfa drugs. The facts produced in this rebutted Testimony support Koch’s conclusions that disease-producing germs can be restored to harmlessness, by re-establishing an effective oxidation catalysis and thus, again be enabled to function harmlessly, in the great biological cycle. This is demonstrated by the fact that, badly infected udders that yield bloody, pusy, milk or very seriously toxic fluid, as milk with bacterial counts running high in the millions, lose their inflamed gangrenous condition fairly soon after receiving the Treatment and yield good commercial milk, with bacterial counts in the thousands and of the same types as those present before Treatment; yet, this milk is not toxic but entirely healthful. The germs moreover linger in higher numbers than normal only so long as tissue debris remaining from the original toxic injury is still present. Thereafter, they disappear and good commercial milk is produced with a bacterial count lower than ordinary. The general health of the cow is improved in a marked degree. The milk production may be increased, the fat content increased, and the reproductive capacity improved. Restoration of tissue function is thus re-established with the restoration of the natural immunity, and Koch’s working Hypothesis that the oxidative production of energy for tissue function depends upon the same oxidative catalysis that converts disease toxins into harmless substances, is still further supported.
During five years of extensive, painstaking, investigation of Glyoxylide as a Treatment for infections in dairy animals by the Department of Agriculture and the Veterinary College of the University of British Columbia, their experts have confirmed both the Theory and practical value of the Koch Treatment, as reported in the Official Report of the Minister of Agriculture to Parliament each year from 1944 to 1948. In March 1948, the final report was printed in the Official Report to Parliament. This Report is in sharp contrast to the hopeless destructionistic report of the Dairy Cattle Health Committee of the American Dairy Science Association, which met at Guelph, Ontario, in the summer of 1947. For Johne’s disease, a fatal form of Para tuberculosis, these dairy experts recommended slaughter of all suspected animals. The British Columbia Report showed that in their experience, the disease was promptly cured by the Koch Treatment. For infertility from Bang’s disease and ovarian cysts, and other causes, cure was established by the Koch Treatment with continuing fertility, and the best of milk production; instead of the great loss to the dairymen of some twenty or more percent of their cattle. For Mastitis likewise, instead of the high steady universal loss of from twenty to thirty percent of the cows, cure and persisting practical freedom from the disease could be gained from use of the Koch Treatment. Thus conservation and constructive gain and saving was proved possible by use of this Treatment instead of the great annual loss of twenty to thirty percent of the cattle because of these diseases they could not control otherwise, and can not even pretend to control by slaughter.
THE CASE OF DR. JOSEPH M. KOLISCH’S SON
“My son, age 18, became ill in July, 1940, in a military camp. I was in Oregon on a vacation and was notified by telephone that the boy had been operated for appendicitis. I returned home and found him in the University Hospital in Culver City as a patient of Dr. Lamont. In spite of the operation being a success, the patient was still under a high fever and the appendix did not show anything. From the complaints, which the boy gave to me and the history, which he had related to me, the diagnosis of appendicitis seemed justified, but there was not any appendicitis at all. He had a high fever and the impression I gained was that it was a septic condition and I treated him and watched him. I treated him conservatively and expectantly for a few days. By conservatively I mean that I did everything to support the system, in view and in the face of an infection, origin unknown. The surgeon and I were on the case at the same time. I tried to establish a diagnosis. A few days afterwards, the location there indicated it was possibly a pyonephritic abscess. That is, an abscess, which might follow an infection, transmitted to the blood, usually caused or often seen after boils or other surface infection.
“This was the working diagnosis at the time. Then, pus showed up in the urine and it was followed somewhat later by a pain, a rather severe pain in the kidney region and then later in the prostatic region and this gradually developed into a condition, which made the diagnosis of a prostatic infection plausible. So, he was treated accordingly.
“In order to arrive at this diagnosis, as I have made this diagnosis, I would never have been able to arrive at it so quickly, had I not taken into consideration the history and I received the history from the patient that he had not been well really for a month prior to this, following an incision of a boil, which developed while he was at the camp there. Following this incision, for a few days he had a fever. He was quite ambitious, so he went back to his duties and he never felt really well after this. Coming down here he thought he had the flu. He saw a doctor. I was not here. Then he went to the beach. He went out one day and the following day he had a severe attack of chills. I took care of him then in the hospital. It was established that it turned out to be mostly septic in nature and I took him to my clinic. My wife used to be a nurse and she took care of him.
“He was in the University Hospital in Culver City for about three weeks. Then he went home to my clinic and he stayed there and things became rather, well, like he had a septic condition. It would seem that he would get a little better and then it would get worse again. He was treated at the time. I had treated him already in the hospital with sulfanilamide and then he received Vitamin B and Vitamin C and liver extracts to keep the blood up.
“Then about the middle of September or so he got quite bad again. The pain got worse and he perspired and it seemed like a new whole thing had started with a new infection again. I was greatly worried, and, having established the diagnosis and knowing the origin of the boil, I thought there was great danger of his developing a heart condition following this thing in a protracted course. Then, it being the genitourinary system affected, I inquired, and I was given the name of Dr. Hagar, as a competent specialist in that line, and he was also seen by Dr. Bacon.
“Dr. Hagar wanted to take him to the California Lutheran Hospital so he took him there and he was under Dr. Hagar’s care. He received sulfathiazole there. I had given him some sulfathiazole at my place already. He was not there very long and I decided to take him back to my clinic. He had symptoms of developing quite a pain in the bladder and the region of the urethra.
“I did not run a metabolism at the time, as I did not think there was any indication. I took all the blood counts, urine, sedimentation, blood cultures, and cultures from the urine.
“The disease was a prostatic abscess infection of the prostatic gland, brought about by way of the blood streams from this boil.
“After he came home he was in very much pain. His fever took a new swing up and I could not see anything but a recurrence again of a general septic condition, which he had already gone through a few times in the course of this disease. He would get better and then get worse, and then get better again, and, while I was always successful in keeping his general condition up, he started to show definite signs of slipping. He was actually sick since sometime in July, and in August he was operated on.
“He had the best of care, but to a man of experience and judgment it was just a matter of time if the resistance of the system would break down and the abscess would appear some other place on the body or a heart condition could have come up. Most anything could have happened. So, at the time, I remembered the Koch claims and Treatments and also the experience, which I had learned and I ordered the Glyoxylide and gave it to him. I telephoned Dr. Koch to ascertain his opinion, what his ideas were and to get a fair impression myself, before I would administer it and to get what he had to say, and what I could expect, and to have as much personal contact as I could. I told him the condition and he told me that he had quite a good experience with similar cases about the prostatic abscess, and then, he told me on the telephone that he expected the abscess to break within seven days.
“The Treatment was administered. The next day, from my observation, the boy was definitely better. He was definitely improved. There was a definite change. The change was one such as you observe at a sick bed. I watched him from the next day on. The boy improved. He had an appetite then. He complained less. He was less nervous and he had less pain. His general condition was definitely improving until the day when the abscess broke, which was the seventh day. It was not a surface abscess. It was the prostatic gland and it showed all physical symptoms possible of being an abscess and it broke and discharged. The pus discharged through the penis and this pus was cultured and it showed Staphylococcus aureus.
“There were repeated blood cultures made but the blood cultures did not show any growth of bacteria.
“On the day the abscess broke, he had quite some pain and after this he was to all appearance well. I kept him in bed, and under close observation, but he was perfectly all right. His temperature was normal. I have the temperature charts taken at the time in my possession and he was all right. He was eating well. He commenced to eat better. Of course, he showed the effects of the sickness but he had no more of the septic condition. The fever never came back again.
“I think the sulfanilamide and sulfathiazole had a deleterious effect on the treatment of this disease.
“I attribute the change which resulted in his recovery to the administration of Glyoxylide.”
THE CASE OF NORMAN REEVES
Paraphrased from the Testimony of Dr. L. L. Andrews
“In the summer of 1940, I had a patient by the name of Norman Reeves. I believe he was about five years old. I was called to him at his home. That was, I believe, June 13th. He had a very high fever. It was around 104° and 105° that afternoon. I saw him around two o’clock or three o’clock with intense pain in his left leg. From his ankle up to the knee it was decidedly swollen and very red and hot and very painful on palpation and I said to the parents, ‘There is undoubtedly infection here in this leg and we want to know whether it is in the bone or not, so I ordered him to the Victoria Hospital for an X-ray of the leg that afternoon.
“He went down there immediately and had the X-ray that evening. The roentgenologist’s report was that there was no involvement of the bone at that time, so it was negative and his report was that there was no periostitis there at all, and from the condition found from this report, I sent the child home, and was called to see him the next day and his temperature was still high, and, in fact, there was a rigidity of the spine. That is, he was stiff. The abdomen was very tender and with the X-ray negative, the apparent condition shifted to the abdomen. It then became a question of whether the original infection was in the leg or in the abdomen. But, after I examined him, I still came back to the leg. I said, ‘I think the trouble is here,’ but I ordered the child back to the hospital and I called in Dr. Barge as a consultant. He came around noon. This was July 15, 1940.
“We saw the child together and decided that our best probability of trouble was in the leg; that we would operate there and if we found nothing there then we would open the abdomen, and the operation was performed and he was my assistant and we let out of that left leg close to half to two-thirds of a pint of pus. We took cultures immediately and it proved to be a pure culture of Staphylococcus aureus.
“We opened the wound practically from the ankle up to about three inches, I think, of the knee and put in drains and put the child to bed with transfusions of blood and local serum solutions and general medical care. The child’s temperature came down after the initial effects of the anesthesia, but there developed, from that infection in the leg, a pyelitis. That is infection in the kidneys. We got a pure culture of Staphylococcus aureus from the urine. Then from the last infection, there developed an infection, which appeared in the lungs and there developed a double infection of both lungs and it went into lobar pneumonia. Then we made cultures from the blood and we got a pure culture of Staphylococcus aureus from the blood.
“I think the records will show somewhere around 10,500 cc. at a time. We were anxious to find, if possible, a patient or some individual who had had a severe case of Staphylococcus aureus infection and had recovered. We were not able to find one. When such a case can be found, a certain degree of immunity develops in that patient and if you can take his blood or get a transfusion from him to your new patient, you get better results than you do with a straight transfusion.
“So as to do all that we could for this child, his brother, a young man, was giving his blood and so he was willing to be treated with the vaccine of this Staphylococcus infection that we got from the little child. So, we treated his big brother with the vaccine made from the infection from the child for somewhere of about ten days, endeavoring to build up in the brother a strong resistance to the Staphylococcus infection. Then we took his blood and transfused it to the child.
“There was at this time sulfathiazole. It was just appearing. My house physician, Dr. Williams, I believe, was her name, who assisted me with the care of the case, said she believed there was a man here in the city that had a little for experimental purposes that had been sent out to him. I said, ‘Well, get it, if you can.’ She succeeded in getting a few grains of it in tablets, and at the same time I wired the manufacturing plant for a supply of the drug for this child. We began immediately to treat this child with the sample that we obtained from this local physician.
“As I recall, we divided the dose about in two, giving him about three or three and a half grains every four hours. The child did not react well. I think it was the second or third day there was a severe rash on the child. That was indicative that he was not taking the drug properly; it was acting as a poison, so we discontinued it until the skin cleared up. Then we tried it again with the same result and we discontinued it and we tried it again. I think the record will show three times. Each time there was a reaction that was indicative that the drug was having a very poisonous effect upon the child and could not be continued.
“During all this time, of course, the wound was properly cared for, dressing it each day, and was cared for by a private nurse. His mother was present all the time. He had first quality care; everything that a good hospital could throw around the child was given, and, so far as I know, everything was done for the child that science could do at that time. The child showed a little clearing of the lungs.
“The records will show his radiograms were made, I do not know how many times, but there are the prints with the interpretations of them and the condition of the lungs showed practically a complete consolidation of the left lung; probably just a little bit of air in the left lung with a little larger space in the right lung, but during the program those conditions began to clear up a little and with every ray of slight improvement, or index of something that might be considered as an improvement, we noted the time on the progress notes. During all of this time, of about three weeks in the hospital, the child was gradually failing, losing in weight; losing in what we call morale, all sense of fighting power; he was becoming intensely weak, refusing food. We were keeping the child alive, apparently, just with a transfusion every two or three days. The parents are not blessed with a lot of funds. The bill had reached somewhere around a thousand dollars and apparently we were running a losing game. The child was getting weaker all the time.
“One day I told the Mother the child would not be able to live and she agreed with me, and I said, ‘You had better take the child home to see what you can do for him at home, or we will do whatever we can. We can’t keep him alive on transfusions forever.’ She agreed to it. So we went home and both of us agreed that the hope for life was practically negligible. Then we tried sulfathiazole again there at the home with the same results, no improvement. He reacted badly to it. We could not give it to him and the child got so weak he could not turn himself over. He could not lift his head. His skin was dry like leather and he was refusing to eat. We had great difficulty in getting a little water down him. So, I said to the father and mother then, ‘There is one other Treatment.’ I advised the parents then to try Dr Koch’s Treatment, and she agreed. So, I wired for a Treatment and I gave it to him. The child showed improvement in twenty-four hours and he was taking water then without forcing it to him, and within forty-eight hours, he was taking food and the improvement was right up the line, getting better.
“The diagnosis was the child was improved, remarkably improved.
“The name of the disease was a pure Staphylococcus aureus infection of the lungs, of the kidneys, of the blood stream, and of the bone. The leg was running pus and it was refusing to heal over the skin wound. That is, there were several foci of infection in there where it was pouring out pus. After the Treatment, or by the administration of this Treatment, there was a marked pick-up in activity of the healing of the skin area, but with the pus coming out, I felt I ought to have another X-ray picture, so I took him to my office and did an X-ray of the leg, and it showed a felucrum of the body section of the bone that had been undermined and was there as a necrotic substance. It is a piece of necrotic bone that has been practically separated from the parent bone, by pus. In such an instance, the wise and simplest thing to do is to remove that piece of tissue bone and so I advised them to go to the hospital and open the wound and curette this out. I took the child to the Jackson Hospital and there opened the wound and thoroughly curetted the bone the entire length of the tibia, from what we call the ephitheseal to the diatheseal line. That was the left leg. The child continued to gain rapidly; he made an uneventful recovery and is sound and healthy today.
“I gave him a second Treatment when he arrived home. The reason for that was this, anesthesia has a deleterious effect upon the activity of this particular synthetic medication. It tends to lower its efficiency, so I gave it to him for another pickup. He made a rapid recovery right on. I have seen him lots of times. I saw him just a few weeks ago; a strong, vigorous, healthy child, and he has never been sick, since. He seems to be immune to everything.
“I think the primary cause for his recovery was this Synthetic Treatment. Now, the surgery was an important factor all right; important that it took away a lot of infection immediately and gave the Treatment a better chance to do its work, and gave the child a quicker recovery.
“I believe the sulfathiazole and other medication had a deleterious effect.”
Mrs. Reeves told of how ill Norman was when they took him home from the hospital. It was because they expected him to die soon and that nothing more could be done for him at the hospital. He was placed in bed so he could see the family for he was too weak to turn or move his head.
They again used the sulfa drug but he was not helped. The rash appeared and grew worse. It was then that Dr. Andrews suggested the Koch Treatment and he phoned for it. It arrived and was injected the next day.
Within twenty-four hours he had improved definitely. He was hungry. His temperature had dropped. That was the first time he wanted anything to eat or had eaten anything, you might say, in the length of time he had been sick. He improved rapidly after that (she explained), and especially after the second injection, and soon was in perfect health.
THE CASE OF MRS. HARDCASTLE PENNOCK
Paraphrase of the Testimony given by Dr. Chester Earl Dove
“I was called to attend Mrs. Hardcastle Pennock along in May of 1941, in Palm Beach. She had a temperature of 104°; pulse very rapid; very much pain in the abdomen; vomiting, and drawing her knees up on her chest. She was attacked with this condition around twelve o’clock at night of May 23rd. She called me the morning of the second. She had had a colonic irrigation. I diagnosed her case to be appendicitis. I based that diagnosis on the temperature and clinical symptoms of vomiting and the trying of a movement of the bowels, which would not move, and the blood count. Without the blood count, we could not have been positive.
“I consulted with Dr. Koch. He came to see her and then I administered 1:4 Benzoquinone. On the twenty-fifth, her temperature went down to 102, as I recall it, and her bowels acted more normally. They had acted hardly at all before that; she passed mucous, and her pain was markedly reduced. She had just the one treatment.
“It will be seen that the white blood cell count dropped about 3,500 cells per day, which is what is generally considered a very big change, (from 16,900 to 10,350 in 48 hours). Correspondingly the toxemia and other symptoms improved, so that on the third day, the white cell count was just a little above normal and the patient had made similar change in her general condition.”
Paraphrase of the Testimony of Mrs. Pennock
“Several years ago I had trouble with my abdomen. I became acquainted with Dr. Johnson. This was about the latter part of May 1941, and he took some blood from me. The night before I was very ill with nausea and very loose bowels. All night long I was in terrible pain, vomiting constantly, and I did not tell my daughter until almost daylight. I was in such distress.
“I have used Miss Touchbarry for irrigation before in my life, so I went over there. It was just at daylight and she gave me an irrigation. She gave me very little water and it did not come back. I was vomiting constantly and in terrible pain. My knees were up. I could not straighten up. She had to go up into one of the rooms and she called Dr. Johnson and Dr. Dove. Dr. Dove had been our physician for many years. He came and called Dr. Koch to see if he could get a Treatment. Dr. Koch came with a Treatment and by that time I had been taken home, in terrific pain, vomiting all the way in the car.
“I omitted one point. Dr. Johnson came and took a blood test.
“Dr. Dove gave me the Treatment and within an hour the pain started to subside and I could straighten my legs a little bit. Within three hours I was comfortable. Up until that time the bowels had not moved again after they had been moving very badly the night before, but about three or four o’clock in the afternoon, my bowels moved again normally without anything administered for them.
“Dr. Johnson came two or three days to take the blood tests and the reports were given to Dr. Dove.
“From that time on I became more comfortable. It was thereafter three or four days until I was in very good condition. I felt much better. I was in bed two weeks. After this two week period, I was up and around and felt fine.”
THE CASE OF GRACE LOEFFLER
Paraphrase of the Testimony given by Dr. A. J. Loeffler
“My daughter, Grace Loeffler, is now twenty-one years old. When she was one year old she had diphtheria, scarlet fever, bilateral mastoiditis, and double lobar pneumonia, all within a month’s period, and very nearly died. She was so sick that nothing could be done at that time about her mastoids. They went un-operated, and she developed, of course, the accompanying otitis media, which is an ear infection.
“Following this attack, for seven years she had a chronic discharging ear, the right one. This ear was always moist in the external canal. The odor of the discharge was very foul. She would find it in her hair and on the pillow. She developed a sort of inferiority complex over the thing, and she was conscious of this odor all the time, and, of course, lost all hearing in that ear. We took her to different doctors, without any results. Some suggested that the only method was a radical mastoid.
“On May 10, 1940, I gave her a treatment of 2 cc. of Glyoxylide. Nothing happened for a period of six or seven weeks, that is, no change took place that I could see. There was no lessening of the discharge, no change in the appearance of the eardrum, which had a perforation for seventeen years. There was no change in odor.
“But after a period of approximately six months, without any more treatment, not even irrigation, this discharge gradually let up, the odor disappeared, and the opening in the eardrum apparently healed over and remained that way for a year and a half, at which time she had a sudden feeling of pressure in her ear and a recurrence of a discharge, but without odor. This discharge lasted about a week.
“She has had three injections over this period of a year and a half. To bring the story to date, she has no discharge from the ear, she can hear a coin click at fifteen feet, and is very happy about the thing because of the fact that she no longer has this dirty, foul, messy, ear. I can only attribute these facts to the fact that the Koch Treatment helped her. This particular disease, from which she had been suffering, is called otitis media chronic, supperative.”
Bronchiectasis
In bronchiectasis, we find a form of infection that appears quite hopeless. Here the infection attacks the bronchus walls, weakening them until they sag and bulge, forming cavities that harbor the infection in a way that is not possible to drain out, except for the overflow of pus, so to speak. Large accumulations of pus developed and are coughed up at intervals, especially in the morning. The bronchus walls are invaded by and generate the infection, serving as foci for its extension further and further into the lung.
The patient is, of course, quite intoxicated by the infection, and the injurious results may affect her in various ways, causing asthma, for example. The hopelessness of the situation is well expressed by Christian in his 15th Edition of Osler “Practice of Medicine,” 1944, p. 814, where he states, “Lobectomy (removal of the affected lobe of the lung) offers the only possibility of cure. Medical treatment is palliative only, since it is impossible to heal the cavities.”
Osler further describes the disease on pages 810 and 813 thus: “The course is long with almost inevitable progression; Exacerbation may follow an acute infection, as a rule, with a superimposed pneumonic consolidation. There may he pleurisy with marked thickening. Hemorrhage is common and may cause death. Septicemia may result. Many patients have a miserable existence from the persistent cough and general ill health. The foul odor of the sputum is distressing to both patient and associates. If definitely established, the disease is incurable by other than lobectomy.” On page 814: “Clearly operation should be advised early, if a skilled surgeon is available.”
Cecil in his Textbook of Medicine, 5th Edition, p. 922, states: “Bronchiectasis is a chronic progressive disease of the bronchi or bronchioles, characterized pathologically by dilatations of the tubes and an inflammatory reaction in their walls, and clinically by chronic cough and expectoration of large quantities of purulent sputum.”
Boyd, in his Textbook of Pathology, p. 463 states: “Moreover, most cases of chronic bronchitis have a basis of bronchiectasis; it is this which prevents complete recovery.”
On page 462: “Although bronchiectasis is usually regarded as the dilation of a bronchus with the formation of a cavity, it is more correct to regard it as an excavation in the lung substance starting in a bronchus. Destruction, no dilatation, is the essence of the process, which results in the formation of an abscess.”
Also: ETIOLOGY, “Suppuration of the nasal sinuses with the constant discharge of septic material into the bronchi is probably one of the major factors. In searching for a cause of septic disease of the lung it is well to look above the clavicle.”
“Chronic fibroid tuberculosis leads to the destruction of the bronchial wall combined with traction on the wall due to the contraction of the fibrous tissue, so that large cavities may be formed.”
“For some unknown reason the left lung is more often involved than the right, and the
lower lobes more often than the upper owing to stasis.”
“The size of the cavity depends upon the size of the bronchus. It is filled with pus that stagnates there owing to insufficient drainage, and still further weakens the wall of the bronchus. The mucosa is hypertrophic and may form tumor-like highly vascular papillary masses. There may be atrophy. The microscopic picture is similar to that of chronic abscess. The mucosa may be hypertrophic or atrophic, and in advanced cases the muscle glands, elastic tissue, and even the cartilage may be replaced by fibrous tissue. The most significant lesion is the destruction of the bronchial musculature and elastic tissue, for it is these, which weaken the wall and allow the dilation to occur. Septic thrombosis may occur with embolism and the formation of a secondary brain abscess.”
It is, therefore, apparent that the recovery from bronchiectasis and its sequel, asthma, following a single injection of a harmless Remedy, must result from a constructive principle at work. Thus the infection state was reversed, the injured walls healed and became strong again. The NATURAL IMMUNITY of the patient’s tissues was re-established, and toxins were oxidized to harmless substance. Even in that act, energy was liberated, and who knows, but that the toxins served a useful purpose through their full oxidation.
THE CASE OF MRS. PEABODY
Paraphrase of the Testimony of Dr. Wendell G. Hendricks
Dr. Wendell G. Hendricks’ Testimony on the Case of Mrs. Peabody can be summarized as follows; she was helped into his office by her husband on January 26, 1944. She was thirty-one years old and weighed only eighty-two pounds. She was in a very severe coughing and asthmatic state at that time. In fact, she had had a persistent asthma attack for days and had not had any sleep. She had dark circles under her eyes and she looked very haggard, very pitiful, anemic-looking; typical of a person that has given up in despair, and gave the history of having this cough and the production of this extreme amount of pus-containing sputum, for many, many, years. That she had suffered with a sinus condition; that the asthma had started three years previous to this time, and that she did not have that in the beginning. The cough was worse in the morning after she had tried to get some sleep on occasions, particularly, if she was able, at all, to lie down this would get worse as she would get up. Most of the time, however, she had to be propped up to breathe.
The examination on that date of the chest with the X-ray confirmed a diagnosis of bronchiectasis, or chronic bronchiectasis with bronchitis, and status asthmaticus, and bronchial asthma, in a continuous form.
“I noticed on my examination that there was a considerable amount of sinus drainage by using the nasal speculum and I felt that an immediate relief could be obtained, if the patient could stand it, by irrigating the sinuses, which I had had some special training in; so, I irrigated the spheuoid and the antrum.
“The antra are located in the cheek and the sphenoid lie deeper at the base of the skull and very often drip down into the throat. This was done on that date.
“The temperature was 100 degrees. The pulse was 130. The blood pressure was down to 100 over 80. It should have been up around 130.
“Her appetite was good in spite of all this trouble, and she could sleep okay, if she were propped up. Between these attacks, she could get some sleep; in fact, she was so exhausted that she would sleep in spite of it, in spite of her labored breathing; and the bowels were okay.
“The red blood cell count was four million and the hemoglobin was 80 percent.
“The patient was given an injection of Glyoxylide on the 28th of January, 1944, two days later; and, she was instructed to have colonic treatments, if needed.
“A prescription was given for visyneral capsules, a combination of vitamins and minerals, one daily.
“On the 19th of February, 1944, approximately three weeks from the injection, she had a three week reaction of chills and fever.
“On the 27th of March, 1944, her pulse was 80; dropped down from 130. Blood pressure was up 12 points to 112 over 80. Her weight had increased 10 pounds. She was 92 pounds. Her temperature, however, had dropped to 99.2 from 100.
“On that date she told me that she had had no asthma since the 19th of February, which was the previous visit three weeks after the injection.
“On the 17th of April, 1944, approximately three weeks later, her temperature was 98, her pulse 72, which is normal, and her blood pressure 110 over 80.
“On the 8th of May, 1944, the temperature was 99.6, and the pulse was 74, which is in the normal range. Blood pressure was 120 over 80, which is absolutely normal for that individual. Her weight was up another pound, to 93 pounds. She had been taking colonic treatments once weekly, due to the extreme amount of pus and mucous, which was producing in the chest and we did not want them to accumulate in the bowel, so we washed that out and we made a notation to continue colonies once weekly.
“On the 29th of May, 1944, temperature normal, 9.9. Her weight, however, had gone down two pounds, to 91; it fluctuated. Pulse 76, normal range. Blood pressure, 130 over 80, still normal range.
“On the 20th of June, 1944, the patient was having relief from her coughing and her asthma, but her sinuses were giving her a considerable amount of pain and on the 20th of June, 1944, on the 3rd of July, 1944, and on the 10th of July, 1944, she was given irrigation of these sinuses, as I did in the beginning, to relieve that congestion and the headache that followed the congestion, which it did relieve.
“On the 4th of August, 1944, there was, I would say, almost a complete recovery of the condition. She had an occasional coughing, but nothing to compare with the original condition; in fact, it was so slight she did not complain about it much, and no asthma. This was the twenty-seventh week after the first injection. As I remember, the patient almost forgot to keep her appointment, as she had a bridge club, and the date slipped her mind, and it certainly impressed me because, in the first place, she was almost beyond going when she first came to me and then to think that she was so well that she forgot to come to see me, impressed me quite a bit as to the recovery she had obtained on this occasion.
“She was given a second ampoule of Glyoxylide on that date, August 4, 1944.
“Now, this patient was seen on, I think, two or three occasions during the year 1945, and she would brisk herself into the office to tell me how she felt and it was that she felt fine; that she did not think she needed any more Treatment; that she did not have any more asthma, and she was not coughing, so she did not see any reason to come to see me. The last time I saw her was either the latter part of February or the first part of March, and she just felt fine.
“I attribute this recovery to the Glyoxylide.”
The X-ray films submitted in court are described by Dr. Omer G. Hague, a noted radiological expert.
TESTIMONY OF DR. HAGUE
(FILM NO. 1)
“This film shows the bony thorax of a rather small female.
“These shadows here are the breast shadows. The central shadow is a long, narrow, poor-vitality type of heart. The left lung is reasonably clear.
“There are some hilar shadows; not more than you would expect in a patient with chronic drainage from the nose.
“The right lung shows exactly the line of the pleura between the two lobes of the lung, between the lower lobe and the middle lobe.
“These soft white shadows in this region are indicative of an infectious process in the active portion of the lung tissue.
“Bronchiectasis is a chronic infection of bronchioles, usually due to a drainage from an upper respiratory tract infection, such as repeated sore throats, repeated sinus trouble with drainage down the post-nasal spare.” (FILM NO.2)
“This shows a little more clearly the outline of the breast shadows and a little better contrast in the type of X-ray showing the dark and the light shadows more clearly in relief. It shows quite definitely that this diseased process in the right lower lung has practically all disappeared.
“The reason that this type of condition more often hits the right lower lung than the left is that the bronchus coming down from the trachea through the right descending bronchus is nearer a straight line than on the left side.
“On the left side it has to go around the right and then up, so that this is a more direct infection into that area.
“But, this film shows that the diseased process has gone away, and that both lungs are almost of equal brilliance.
“In my opinion as a radiologist, the change in the condition (Mrs. Peabody from January of 1944 to August of 1944 represents a favorable recovery process, definitely.”
AN ANALYSIS OF THE REBUTTAL OF THE PEABODY CASE ATTEMPTED BY DR. BRUCE DOUGLAS
Dr. Douglas gave the rebuttal “opinion” that bronchiectasis in this case got well because Dr. Hendricks washed the nose out a few times and that bronchiectasis gets well anyway. This “opinion” is contrary to the facts in this case since the bronchiectasis had continued for many years progressively getting worse and the X-ray shows that large portions of the lungs were involved.
According to the authorities quoted, and these are the leaders in medicine, recognized by all, the affected part of the lungs must be removed surgically to obtain a cure. No other Treatment is effective in this progressive disease, once it is established. It must be also pointed out that irrigation of the sinuses a few times does not remove the infection from them, for the walls are injured in much the same way as they are in the bronchi and the germs develop in pockets within the walls that are not accessible to an irrigating solution. The walls of the sinuses and of the bronchi generate the infection. If any trickles down into the lungs from the sinuses, it only adds to the pus that is overflowing from the cavities within the lungs themselves. Thus, the pus added from the sinuses only increase the overflow from the lungs and does not cause it.
By referring to the statement of the authorities, the error of Dr. Douglas’ rebuttal should become evident.
It would be well to point out that surgery would have no place in this case. One-half of the right lung, at least, would have to be removed. Probably also one-half of the left lung. A woman so depleted who couldn’t get her breath would have little chance of sustaining such an operation.
THE CASE OF DR. F. F. WOODRUFF’S SON
Paraphrase of the Testimony of Dr. F. F. Woodruff
“I have used the Koch Treatment on my son. He was afflicted at the beginning with a severe cold, and it developed into recurrent oposthotons (convulsions), infection with involvement of the ears. The middle ear was involved to the extent that both drums were lanced. I called into consultation a friend of mine to assist me in this case. The boy had to be given sulfathiazole, and he gradually become worse. He became unconscious, and we were all quite concerned as to the outcome. I wired Dr. Koch, and an injection of Glyoxylide reached me the next day. He gave definite symptoms of meningial involvement. We term that condition as opisthotonus, which is from brain irritation, meningial irritation; He was unconscious and running a temperature between 103 and 104 continually.
“I noticed changes the evening following the morning that we administered the Treatment. He showed some signs of improving. The next day he was conscious, and he made a rapid recovery. I attribute the recovery to the Koch Treatment.
“I would say that I rely on Dr. Koch’s Treatment in those stubborn resisting cases, the various types that we run into. Many cases that will come to me do so on account of my profession, to avoid surgery. I have had several such cases, so I will resort to this Treatment in my effort to avoid surgery, as in goiter, and cases of chronic synovitis, where they have been recommended to me. I have had some results in cancer cases. We get some very bad cases referred to us by other satisfied patients from cancer. My opinion is that there is a definite value in Dr. Koch’s Treatment.”
Rheumatic Fever
THE CASE OF EDNA NEWTON
Paraphrase of the Testimony of Dr. Wendell G. Hendricks
“Edna Newton, age 11. Joints were painful, hot, swollen. Knees were the worst. There was high fever, sore throat, and pain over the heart. These symptoms had progressed five days previous to the visit to my office. There was contraction, swelling of all the joints causing the limbs to be markedly flexed. Heart murmur, pulse 120, temperature 102, throat inflamed, tonsils swollen, and severe adenoiditis. Diagnosis was acute rheumatic fever. July 3, 1942, the girl was put on a liquid diet and given an injection of 1:4 Benzoquinone. The next day the temperature was 100, pulse down to 108, her throat and knees were better. Two days later, temperature 99.2, pulse 100, throat clear, all joints better.
“July 9th, 1942, all joints normal, normal function, no pain or swelling, temperature 98.6, pulse 78, throat normal. Heart murmur gone. Adenoiditis gone. Patient is well.
“Rheumatic fever is one of the diseases for which no treatment has been developed, which has any beneficial effect except the Koch Treatment. We are happy in having had all of our Rheumatic Fever cases respond very well to the Koch Treatment. Since, this disease generally leaves some sequel that in later years rises up to threaten the health or life of the patient, it is indeed gratifying that the Koch Treatment gives prompt and completely satisfactory results in the cases where it has been used so far.”
TESTIMONY OF MR. SHEAD NEWTON
“My wife was working when our little girl got sick and we sort of neglected her. I thought she had probably been stung by a bee. Her ankle swelled up to the knees and then her joints and she got to drawing and just sort of pulling together, her feet and head coming together. The third day after Dr. Hendricks gave her the shot, I am almost positive that her temperature was back to normal. It was no time until the swelling and everything was gone and she was coming along fine.”
TESTIMONY OF MRS. SHEAD NEWTON
“In July, 1942, my daughter, Edna, 11 years old, was ill a week before we took her to Dr. Hendricks. She could not stand on her feet. Her feet and hands were drawn, her heart beat too fast, and she had a fever. She complained of her throat. After the Doctor gave her the injection, the first morning we did not notice any difference. The second morning she had no fever and the third morning she was really lots better. She was in bed another week and the third week she was able to be up and around. She has had perfect health since then. We have never had her back to the Doctor for anything. Her heart seems to be all right. She is a little nervous yet, but nothing like she was before we took her to the Doctor. She does not shake at all.”
Advanced Rheumatoid Arthritis
THE CASE OF LUCILLE JAMISON
Paraphrase of the Testimony of Dr. Wendell G. Hendricks
“Lucille Jamison, age sixty, February 6, 1941. Six years ago fell on tile floor and injured right knee. Arthritis started in both knees and progressively became worse. A year later developed nodules of the popliteal fossae and subcutaneous nodules of the hand. Examination showed arthritic process of the metacarpal phalangeal joints with atrophy of the muscle between the thumb and first finger. Hyperthropic arthritis of both knees very marked, swollen, subcutaneous nodules, one in the tissue of the dorsal surface of the right hand, and one in the popliteal space. There was general inflammation and general disability of all her joints.
“February 9th she was given Glyoxylide. She had a local reaction after this injection. There was a definite improvement, a limbering up of the joints. October 3rd a Treatment of Benzoquinone. January 7th, 1942, I noticed a small nodule forming in the left hand on the dorsal surface. The nodules had all disappeared on the right hand and the back of her knees and her joints were practically limbered up. I felt that she had had as much recovery as she was going to get, but after a temporary enlargement of the joints and another reaction of fever I gave her another injection of Glyoxylide February 20th.
“After the third injection, Mrs. Jamison was so well that she just felt like she would never need any more. She was doing her own housework and walking uptown where before she had been in a wheel chair and had to be helped all the time, helped out of bed and suffering all the time.
“The fourth and fifth injections were given at the yearly interval from the last injection because it seemed that about once a year there would be a little stiffening of the joints. Even. though the patient was out and around doing her normal occupation, I gave her an injection. She is in good shape. She has recovered.”
TESTIMONY OF LUCILLE JAMIESON
“My trouble started about ten years ago and got worse all the time. Finally, I could not get up without assistance, could not raise my hands up, and could not wear shoes. My ankles were swollen and my hands were deformed. I could not hold anything in my hands, turn my head, or raise my arms. I had been doctoring with no results from May 1934, until I went to Dr. Hendricks in February 1941. He put me on the Koch Diet and then gave me the injection. In about ninety days, I got to feeling much better. My joints limbered up and the pain started to go away. That burning sensation was gone. It has been disappearing ever since until it is gone. I feel very good, get around well, and do my own work”
Eunuchoidism
Joseph S., fourteen years old, was brought in by his sister, Dr. S., a physician. He was considerably overweight and had the shape characteristic of the female, narrow shoulders, big hips, also the fine hair, soft voice, and the general impression of a girl. Examination revealed that the penis was infantile, the scrotum very small, merely a fold of skin and empty. The testicles were not present in the scrotum, nor could they be palpated in the canal. It was evident that this was a case of total eunuchoidism—the most extreme form of primary genital insufficiency. True eunuchism is where the sex glands are removed surgically or destroyed.
Both maladies are recognized as incurable. In extreme eunuchoidism, the glandular system that is defective involves not only the sex glands, but also the pituitary and others. There is no known way of restoring the deficiency so that a normal development can take place. However, the use of gland extracts and synthetic products may help reduce the female appearance to a little extent, but very slightly if at all; but the development of the testes and sex organs is not helped. So true is that that Meachin states in his text, “The Practice of Medicine,” p. 862-8 65—’ ‘the treatment of primary genital hypo-function is almost as unsatisfactory as in the eunuch.” Since the eunuch has no testicles to stimulate or act upon, medical treatment is useless and so with this extreme form of eunuchoidism; whatever rudiment of testicle tissue that might be present in the body, it is not sufficient to show any effect of stimulation by gland therapy.
However, the inhibitative agency that prevents the proper development of the glands is present in a dominating way and what is needed is to remove it if normalcy is to be attained. Then nature can go ahead and complete the development of the pituitary and testes to their normal design and structure. What the nature of the inhibitative agent is appears quite clearly from the fact that it is destructible by oxidation inducible through an auto-oxidation. It thus belongs to the class of substances that are causative to both allergies and anergies, to cancer, and to hyperthyroidism, hypothyroidism, etc. It is able to act as an oxidation inhibitant and allow food material to accumulate as fat instead of being burned to produce energy. And it belongs to the class of fluorescent substances that can transfer energy away from chemical systems where it belongs, to systems where it does not belong. It may thus resemble the viruses and some other parasites in their means of obtaining energy or delivering it from where it belongs, according to Dr. Koch. In this way the tissues of the urinogenital ridge may be deprived of the energy required for their development, and when the interfering substance is removed, normal development can progress.
(Author’s note: The boy was given a dose of Glyoxylide about fourteen years ago. He began to change very soon. In twelve weeks, he showed a marked development of the sex organs and his physique changed. In another three months, he was totally normal. The testes had fully descended and were large and firm. The penis was fully developed. He grew much taller; lost his fat hips, and his shoulders and jaws developed. He became a veritable “Marine.” Years later during the war he joined the Marines and became a Corporal, is married and has children that are normal. This case should be studied closely as a pattern of a group of similar type.
The case is described by Dr. S. as follows:
“I am an osteopathic physician and surgeon. I practice in Detroit. I have a brother, Corporal Joseph S., age twenty-seven. He is approximately ten years younger than I am and I helped take care of him when he was a young boy. He is now in the United States Army at the Army Law College in Washington,
“When he was twelve or fourteen years old I took him to Dr. Koch for examination. He was very obese for his age and we were rather worried about his condition because he was always backward in school, also his general condition was bad. His genitals were not developed as they normally do in a boy that age. His testicles had not descended and the penis was very small; it was almost infantile. He did not respond to endocrine therapy.
“Dr. Koch was consulted and gave him an injection, and within three months he lost weight and his left testicle began to descend, and within the next three or four months they both had descended; his penis grew out. He grew taller and mentally he was more alert. His health is excellent. He is living a happy, normal sexual married life.”
Toxic Nodular Goiter
Mrs. M. Jones
Mrs. M. Jones, age thirty-five, in July, 1943, was examined by Dr. Julian F. Baldor of Tampa, Florida, and found. to have lost considerable weight, and to have suffered recently from excessive nervousness, tremor, pains in the legs, terrific heart palpitation, shortness of breath, and such extreme weakness that she had to be carried into the car to be brought to the doctor. The blood pressure had risen to 190 over 110, indicating a general sclerotic and dangerous hypertension. There was throat constriction and muscle twitching.
Examination revealed a woman with well-developed tremor and muscle twitching, exophthalmus, tachycardia, loss of weight and strength, nodular thyroid enlargement. The basal metabolism rate was 104, July 8, 1943. The heart failing. The systolic pressure in the next few weeks dropped to 170, while the heart heat became weaker and the diastolic pressure stayed up to 110, showing the fundamental toxic state was not abating. (Plate 34)
PLATE 34. The laboratory report of La Beneficial Espanola, in the Case of Mosetta Jones showing that her basal metabolic rate was plus 104%.
From July 8 to November 10, 1943, iodine was tried with absolute rest and ice packs to the thyroid gland, but the condition steadily grew worse. She was inoperable. The iodine (which is only useful for a short time and which is only applicable to certain cases and not to the nodular type of toxic goiter) was not succeeding in preparing her for operation and the heart had to be protected from further toxic injury. The nodules on the thyroid kept increasing.
Therefore, since she could not be operated, the Koch Treatment was used. Two c.c.’s of Glyoxylide was given intramuscularly, and, in a few days, one could see that the trend of the disease was reversed. The tremor improved, the heart beat stronger, she could soon get around on her own strength; the whole picture steadily changed so that by the end of the twelfth week she was back to work, a normal woman. The tremor was gone, the exophtalmus was gone, the nervousness was gone, the blood pressure was normal, 145/90, and later 140/80, had strength instead of weakness. The heart rate was 80 to 90. The thyroid was normal in size and the nodules were gone. Instead of being carried and helped, she was on the go, working.
Her basal metabolism, March 16, 1944, was a very fine normal, namely plus 6. (Plate 35)
PLATE 35. This is a metabolism report from the Laboratory of Clinical Pathology showing that Mrs. Jones’ basal metabolic rate, after the Koch Treatment, was a fine normal “plus 6%.”
This was an instance where a life was saved which could not be done in any other way as experience shows. Moreover, instead of removing or destroying an important organ, it was made normal by removing the toxic cause of its pathology. This, too, was done in a physiological way. More than this was accomplished, the cause of the thyroid disease was the cause of an arteriosclerosis that affected the body in general, and it caused other injuries. The removal of this fundamental toxic agent, by a process of body cell normalized oxidation is an ideal accomplishment in medicine that speaks volumes of hope for future medicine.
THE TESTIMONY OF MRS. MOSETTA B. JONES
“I used to have a dance orchestra but I had to give it up. My hands became useless. I could not play the piano any more. That was in February, 1943. First, my trouble started in my fingertips with throbbing. It seemed as if the blood circulation was half stopped. My hands began to swell and I could not wear my rings at all. I had terrific pains, and then I began having trouble with my legs. It went from one bone to the other. I began to have contractions of the muscles. My toes would draw up into knots. I was in such pain I could hardly stand it.
“I went to Dr. Baldor about it. He gave me first one thing and then another, but I did not improve any. He sent me to the clinic to have a metabolism test made, and after that started a different treatment. It was some drops. All the time I was taking on like crazy. I could not sleep at night; my husband had to lift me up in bed. My hands and legs got steadily worse. Finally, I got so bad my husband had to pick me up and put me into the car. I could not get in; my legs would just turn to water.
“I went back to Dr. Baldor, and he gave me the Koch injection. About two or three weeks later I felt like a new woman. My strength came back, my legs and hands cleared up, and I can use them again. I now have a job demonstrating. I carry a suitcase weighing fifty pounds in and out of homes.”
Hay Fever and Hemorrhage Urticaria
THE CASE OF MRS. WANDA L. RYAN
Paraphrase of the Testimony by Dr. Wm. F. Koch
“I treated Mrs. Ryan in May, 1934.
“She had a multiple allergy and it expressed itself in a multiple of ways too. She had hay fever intensely. She had asthma. She had Urticaria of a hemorrhagic type, that is, the blisters that developed on her were bloody. Then, she had a bowel disturbance that went with it. She would blow up with gas and passed volumes of gas from her rectum. Besides that, there was a urinary disturbance.
“She had been under the treatment of someone at the University of Michigan Hospital, who had arranged a very skimpy diet for her which she was on, but her symptoms were just as bad anyway. They had made a number of tests, which, from the history, at least, would show that she was allergic to sixty or so different things.
“I gave her a dose of Glyoxylide, and, in the course of a month, she was very much improved; and in the course of three months, she made a complete recovery.
“She was allowed to eat anything on the list that I recommended. Yes, that was the Koch Diet, but she went beyond that and ate other things.”
(Authors’ Note: It would be interesting to many to know that Mrs. Ryan still claims full freedom from her illness—in 1948. Can any other Treatment accomplish this?)
TESTIMONY OF WANDA L. RYAN
“I had a condition which was very bad. It lasted about a year and a half. It was like a severe hay fever. I was constantly sneezing, and had a discharge from my nose. It was naturally worse at times than others, but I was never entirely free of it during that time, in the morning, when I awakened, and it usually took until noon before it cleared up. There were days, usually these periods lasted for two weeks, when I would be so miserable, I just could not do anything else but attend to my nose. My eyes would water and I just could not breathe. I just was not fit to do anything but look after myself during that period. I became very discouraged.
“Blotches would appear on various parts of my body, fairly good sized, dark in color, maybe kind of a reddish blue. They were distressingly itchy at first, and then the itch would disappear after six weeks or more, that is, that severe itching, but the blotch would stay there a year and in many cases, two. It did not appear on my face. These blotches were sort of pusy like at first. They would eventually dry. I had very much trouble with my bowels.
“August, 1933, I went to the University Hospital. They gave me skin tests and put me on a diet. There were sixty different things to avoid. In the spring of 1934, I went on a trip and I was very, very miserable. There were nights when I could not sleep at all; and when I was in the car, I just had no relief whatsoever all day long.
“In the meantime, Dr. Koch had come back from Europe and gave me the Treatment. I took another trip after the injection, about three weeks after, and I decided to eat what I wanted to. From that time, I have been able to tolerate anything and sleep on feathers and have a cocker spaniel. I began to have beneficial results within a month. It was perhaps two months when I was entirely free.”
Coronary Thrombosis
THE CASE OF DR. HENRY C. ARNOTT
Paraphrase of the Testimony by Dr. David H. Arnott
“On December 8, 1936, I treated my brother, Henry, for a very commanding seizure of coronary thrombosis and I gave him Glyoxylide.
“The following indicated he had coronary thrombosis. The history of walking down Young Street and being seized in Toronto a few days before with a pain in the center of his chest, which passed off when he rested, but this attack came on while he was sitting quietly in his own home, and it was not relieved by resting and was a very, very, severe attack, and the pain was there in spite of giving him morphine to make him unconscious. When he came out of the influence of the morphine, the pain was still there and the pain was in the center of the chest. My brother said it was a terrible pain; it was a terrible pain. My brother is a brave man. That is the diagnosis, sir, and he looked very ill.
“The Glyoxylide gradually relieved his pain and eventually he got up and around, and I am sure that the turn for the better came because of the use of the Glyoxylide.
“Electro-cardiograms were taken of my brother. They were taken sometime after I gave him the Treatment.”
(The documents referred to were marked Respondent’s Exhibits No. 179 and No. 180 for identification.) (Plates 36 and 37)
“Yes, these exhibits are the electro-cardiograms.
“No, I did not arrange to have them taken. These men were interested in my brother, and came out and took them, and it was all right with me.
“From the standpoint of my brother’s condition at that time, I do not think that rest alone in bed would have brought him around. I say this because of the severity of the attack, the type of the attack. I think he would have died in a very short time.
“Coronary thrombosis is a common disease today. It is more frequent now than it was ten years ago. The vital statistics from Canada for ten years, as of 1940, show that 455 deaths take place out of every thousand due to angina pectoris and coronary thrombosis.”
PLATE 36. The above is an electrocardiogram made five weeks after the Koch Treatment when pain was entirely gone, January 15, 1937, in the Case of Dr. Henry C. Arnott.
TESTIMONY OF DR. HENRY C. ARNOTT
“I live in Burlington, Ontario, am seventy-two years old, and retired from practicing medicine about six or eight years ago. I am an M.D. Received my medical training in part at Western University in London, Ontario, and graduated from the Detroit College of Medicine in 1898. I also got a degree in Edinburgh Medical School in 1898 or 1899. I practiced in Marlett, Michigan, and then I practiced in Hamilton, Ontario, most of the time. Dr. David Arnott is my younger brother.
“A few years ago I was in industrial medicine, and feeling as well as usual. I went to Toronto one day to get myself examined, and I had an attack on the street. I had a very severe pain in the pit of my stomach. I had to stand still to catch my breath. I had just had lunch, and thought it was acute indigestion. It passed off in a few minutes, and I went to the oculist’s to have my eyes examined. I went home that night, and went to work the next day, feeling as well as usual. “Four or five days later, at dinner, I had a very severe pain in my stomach near the end of the meal. The pain was so terrific that I had to crawl upstairs on my hands and knees. My wife prepared a hypodermic, and I took a half-grain of morphine by hypodermic.
PLATE 37. The above electrocardiogram was taken eight weeks after that shown in Plate 36, indicating that recovery was established.
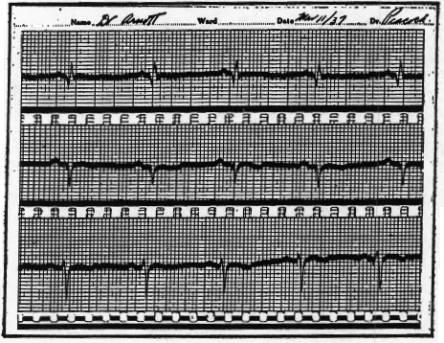
“My wife called my brother in London, and he came and gave me a hypodermic. I was in bed after that for practically four months before I was able to get out.
“In the light of what had happened to me, I realized that I had had several attacks. I did not know that I had an attack of coronary thrombosis when I was in Toronto. I thought I had an attack of acute indigestion, but in the light of what happened after that I am quite sure my previous attacks were heart attacks.
“This attack, when I was in bed four months, was preceded by a pain in my stomach. That epigastric pain was the dominating thing in my life. It was terrific, and the morphine I took didn’t relieve me at all, as far as my sensations were concerned. There was no other pain. This pain in my stomach led me to diagnose my trouble as coronary thrombosis. Pain in the epigastric region is very often indicative of that.
“My brother told me that he had given me Glyoxylide when he came and gave me an injection at the time of that attack. I don’t think I could say that I could notice any change in my condition, I was too sick.
“In my own practice, I don’t think I have seen any case as severe as mine. From my experience, I thought I was through. I think that the rest in bed helped considerably, and I don’t think there is any doubt that the Glyoxylide had something to do with it. I was very careful of myself for a time after that. I retired completely.
“I haven’t had any attacks since then. At the present time I am quite active. I am a gardener in the morning. I do a good deal of walking, and go up and down stairs as frequently as I like without any apparent discomfort. In fact, I think I am a pretty healthy man for my years.”
Psoriasis
THE CASE OF HENRY W. COLE
Paraphrase of the Testimony by Dr. Chester Earl Dove
“I am an Osteopathic physician and surgeon and have practiced in West Palm Beach since 1919. Henry Cole came to me in July 1934. He was suffering from a condition we call psoriasis. He was in very much pain, complained about not sleeping. His skin, in places, was as dark as the ace of spades. In spots, where the epithelium had died and broken away and on other places on his back and body, the blood would come through his two shirts. He had large scales and when he would take off his shirt they would come off and fall on the floor.
“This condition was all over him, from his head to the bottom of his feet; his eyes, eyelids, ears, privates, and every other place, not a fraction of an inch apparently that was not covered. I put him on a diet for a few days and then gave him Dr. Koch’s injection, Glyoxylide. I consulted with Dr. Koch about the patient’s condition.
PLATE 38. The “before and after” pictures were made of Henry W. Cole who made a complete recovery from psoriasis after the Koch Treatment was administered, according to sworn Testimony.
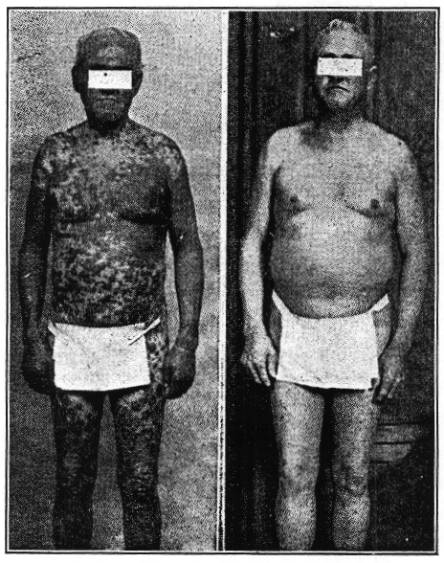
“He had some wonderful reactions as time went on, in a few months, he began to clear up at times and then he would have a reaction. During his bad reactions, that first six or eight months, you would think the man was getting worse, because it draws the poison out apparently and cleans out the system. Then he would get better, and he kept on that way until he was well. In October, 1934, I gave him another injection and have given him one every year or so since.”
(Note: This testimony was given before the Federal Trade Commission hearing held at Palm Beach, Florida. Dr. Dove saw Mr. Cole in January, 1948, and stated that Mr. Cole appeared to be free of his former disease, and in good health.)
TESTIMONY OF HENRY W. COLE
“I am 73 years old and a lumber mill worker. In 1931 or 1932, I began to have trouble with my skin. It came on gradually, first spots and it got all over me. I felt mighty bad. I would scratch it hurt. I was nervous and would jerk. I was covered from the top of my head to the soles of my feet. I went from one doctor to the other. They gave me medicine and violet ray, but they did not help me. Dr. Brantly gave me a letter to Dr. Dove.
“Dr. Dove had photographs of me. The skin on both arms and under my chest was perfectly red and mostly scaly, but the smooth part looked like a raw piece of beef. My fingernails came off; the bottoms of my feet came off, the whole sole. It was just like ripping off a shoe sole and I had to take it out and bury it, it was so large.
“I could not sleep. When I lay down, it was like lying in a bed of ants, and they seemed to be all over me. Dr. Dove gave me several injections, the first around the 17th of July 1934. I just gradually got better, and about a year later, the condition was all gone, and it has never recurred.”